Download
1 / 28
280 likes | 380 Views
<?xml version="1.0"?><AllQuestions />. <?xml version="1.0"?><AllResponses />.

E N D
<?xml version="1.0"?><AllQuestions /> <?xml version="1.0"?><AllResponses /> <?xml version="1.0"?><Settings><answerBulletFormat>Numeric</answerBulletFormat><answerNowAutoInsert>No</answerNowAutoInsert><answerNowStyle>Explosion</answerNowStyle><answerNowText>Answer Now</answerNowText><chartColors>Use PowerPoint Color Scheme</chartColors><chartType>Horizontal</chartType><correctAnswerIndicator>Checkmark</correctAnswerIndicator><countdownAutoInsert>No</countdownAutoInsert><countdownSeconds>10</countdownSeconds><countdownSound>TicToc.wav</countdownSound><countdownStyle>Box</countdownStyle><gridAutoInsert>No</gridAutoInsert><gridFillStyle>Answered</gridFillStyle><gridFillColor>255,255,0</gridFillColor><gridOpacity>50%</gridOpacity><gridTextStyle>Keypad #</gridTextStyle><inputSource>Response Devices</inputSource><multipleResponseDivisor># of Responses</multipleResponseDivisor><participantsLeaderBoard>5</participantsLeaderBoard><percentageDecimalPlaces>0</percentageDecimalPlaces><responseCounterAutoInsert>No</responseCounterAutoInsert><responseCounterStyle>Oval</responseCounterStyle><responseCounterDisplayValue># of Votes Received</responseCounterDisplayValue><insertObjectUsingColor>Red</insertObjectUsingColor><showResults>Yes</showResults><teamColors>Use PowerPoint Color Scheme</teamColors><teamIdentificationType>None</teamIdentificationType><teamScoringType>Voting pads only</teamScoringType><teamScoringDecimalPlaces>1</teamScoringDecimalPlaces><teamIdentificationItem></teamIdentificationItem><teamsLeaderBoard>5</teamsLeaderBoard><teamName1></teamName1><teamName2></teamName2><teamName3></teamName3><teamName4></teamName4><teamName5></teamName5><teamName6></teamName6><teamName7></teamName7><teamName8></teamName8><teamName9></teamName9><teamName10></teamName10><showControlBar>All Slides</showControlBar><defaultCorrectPointValue>0</defaultCorrectPointValue><defaultIncorrectPointValue>0</defaultIncorrectPointValue><chartColor1>187,224,227</chartColor1><chartColor2>51,51,153</chartColor2><chartColor3>0,153,153</chartColor3><chartColor4>153,204,0</chartColor4><chartColor5>128,128,128</chartColor5><chartColor6>0,0,0</chartColor6><chartColor7>0,102,204</chartColor7><chartColor8>204,204,255</chartColor8><chartColor9>255,0,0</chartColor9><chartColor10>255,255,0</chartColor10><teamColor1>187,224,227</teamColor1><teamColor2>51,51,153</teamColor2><teamColor3>0,153,153</teamColor3><teamColor4>153,204,0</teamColor4><teamColor5>128,128,128</teamColor5><teamColor6>0,0,0</teamColor6><teamColor7>0,102,204</teamColor7><teamColor8>204,204,255</teamColor8><teamColor9>255,0,0</teamColor9><teamColor10>255,255,0</teamColor10><displayAnswerImagesDuringVote>Yes</displayAnswerImagesDuringVote><displayAnswerImagesWithResponses>Yes</displayAnswerImagesWithResponses><displayAnswerTextDuringVote>Yes</displayAnswerTextDuringVote><displayAnswerTextWithResponses>Yes</displayAnswerTextWithResponses><questionSlideID></questionSlideID><controlBarState>Expanded</controlBarState><isGridColorKnownColor>True</isGridColorKnownColor><gridColorName>Yellow</gridColorName></Settings> <?xml version="1.0"?><AllAnswers /> ACA Implementation Update:Exchanges, Medicaid Expansion and Essential Health Benefits September 20, 2012 Health Policy Alternatives, Inc.
Overview • Health Insurance Exchanges • Status of State implementation • Medicaid Expansion • Implications of Supreme Court Ruling; State activity • Essential Health Benefits • Federal implementation status; State activity Note: This presentation reflects HPA’s current understanding of the law and the status of federal and state implementation efforts. HPA views may change in the future, and government entities may hold different views. Health Policy Alternatives 9-20-12
Health Insurance Exchanges: Federal Implementation Activities • Final rule on establishment of Exchanges published on March 27, 2012 (some provisions interim final) http://www.gpo.gov/fdsys/pkg/FR-2012-03-27/pdf/2012-6125.pdf • Blueprint for approval of State Exchanges -- August 14, 2012 http://cciio.cms.gov/resources/files/hie-blueprint-081312.pdf • Guidance on the federally-facilitated Exchange published May 16, 2012 http://cciio.cms.gov/resources/files/FFE_Guidance_FINAL_VERSION_051612.pdf • Grants to states http://www.healthcare.gov/news/factsheets/2011/05/exchanges05232011a.html Health Policy Alternatives 9-20-12
Review of Exchange Basics • Basic Exchange functions • Eligibility and enrollment • Consumer assistance • Certify plan offerings • Three alternative approaches to establishing Exchanges • State-based Exchange • State may use Federal government for some activities • Federally-facilitated Exchange (if State elects no) • State Partnership Exchange • State certifies plans and/or provides consumer assistance • Exchange decision not a one-time event; a State may later elect to begin Exchange (e.g., 2015, 2016) Health Policy Alternatives 9-20-12
Exchanges: Key Deadlines • November 16, 2012: States submit blueprint for federal approval of Exchange • January 1, 2013: HHS will approve or conditionally approve state-based exchanges • October 1, 2013: Initial open enrollment period for Exchange coverage begins (through February 28, 2014) • January 1, 2014: Coverage sold through Exchanges becomes effective Health Policy Alternatives 9-20-12
Federal Grants to States for Exchanges • Planning grants: All States except Alaska received Exchange planning grants. • Early innovator grants, IT infrastructure: Four states and one consortium (MD, NY, OR, WI, and a consortium of the six New England states) received early innovator grants • KS, OK applied and awarded but then turned down funds • Establishment grants: To date, 29 states have received establishment grants; 6 have been awarded Level Two grants which require legal authority for Exchange, governance structure and commitment from governor to proceed. • Regular deadlines for new funding applications have been announced (up to October 15, 2014) • http://www.healthcare.gov/news/factsheets/2011/05/exchanges05232011a.html Health Policy Alternatives 9-20-12
15 States + DC have established Exchanges 3 States pursuing Federal-State partnership Exchange 7 States have decided not to create Exchange 16 States studying options No significant activity in 9 states Status of State Activity on Exchanges(July 2012) Source: Kaiser Family Foundation, “State Action Toward Creating Health Insurance Exchanges,” as of July 30, 2012
State Exchange Activity • Exchanges established: legislation enacted, governance established, other activities underway (15 states & DC) • CA,CO,CT, DC,HI, KY,MD,NV,NY,OR, RI,VT,WA,WV • MA and UT have pre-ACA exchanges • Decision against state exchanges: federal grant funds returned in some cases (7 states) • AK, FL, NH, LA, ME, SC, TX • Partnership model (AR, DE, IL) • Uncertain (25 others) includes cases where Governor and legislature (or in KS, insurance commissioner) disagree over building Exchange; ballot initiative in MO; others postponed until after election (e.g., WI). Health Policy Alternatives 9-20-12
Federally-facilitated Exchanges • May 2012 guidance emphasizes preserving traditional responsibilities of state insurance departments and harmonizing with state laws where possible • FFEs will be open to any Qualified Health Plan that meets the certification standards (at least for the first year) • Potential concerns • Relationship between FFE and Medicaid/CHIP programs for seamless eligibility interactions (e.g., IT platforms, data sharing agreements, timeliness and notifications of determinations) • Conflicts between state laws and FFE certification requirements Health Policy Alternatives 9-20-12
Supreme Court Decision • “Mandate”: upheld penalty on those without coverage as a tax • Medicaid: • Rejected Medicaid expansion as a mandatory coverage group (rejected application of statutory penalty of withdrawal of all federal matching funds for State non-compliance.) • Effectively retained Medicaid expansion as a state option, including the higher federal matching • Rest of law: upheld all other provisions of law Health Policy Alternatives 9-20-12
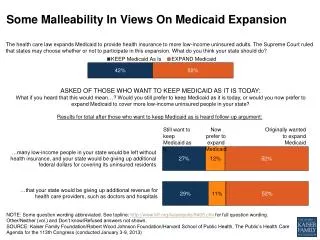
Medicaid post-Supreme Court:What do we think weknow? • Outcome of the Court decision on Medicaid coverage is uncertain • States can: • Implement full Medicaid expansion to 138% of FPL, or • Refuse to implement Medicaid expansion, without penalty • That is 15 million individuals total (Urban Institute) • State can implement in 2014 or implement in later years. If delay, matching rate does not roll forward (100% for 2014-2016, phasing down to 90% by 2020) • If State fails to implement: • Those between 100% -133% of FPL can still get sliding scale subsidy in Exchange : that is 3.5 million individuals • Those below 100% of FPL have no source of subsidy: that is 11.5 million individuals • The rest of ACA remains in place Health Policy Alternatives 9-20-12
What don’t we (yet) know? • HHS has not yet spoken about implementation • Can State pursue partial expansion? • Negotiate sub-population (i.e., up to 100% of FPL)? • Negotiate different services, approaches? • Implement in some counties but not others? • Can State phase? • Preliminary reading of law by many is that it may be “all or nothing” option: so what incentives/tools does Secretary have? • Interpreting statute? • Waivers? (budget neutrality issue) • What are unknown/unknowns? For discussion of issues, see Sara Rosenbaum and Timothy Westmoreland, “The Supreme Court’s Surprising Decision On The Medicaid Expansion: How Will The Federal Government And States Proceed?”, Health Affairs, August 2012. http://content.healthaffairs.org/content/31/8/1663.full.html Health Policy Alternatives 9-20-12
Given Supreme Court decision and State politics, it is necessary to look at Medicaid expansion over period of time • Pre-November, 2012 – Election – political posturing – HHS determines framework/States begin to negotiate • Post-November, 2012 through early 2013 - States sort selves: Health Policy Alternatives 9-20-12
* Includes 50 States plus District of Columbia Source: Kaiser Family Foundation, “Historical Review of How States Have Responded to The Availability of Federal Funds for Health Coverage,” August 2012. Health Policy Alternatives 9-20-12
Congressional Budget Office (CBO) Update Based on Supreme Court Decision One way to look at potential implementation issues is through CBO projection of change in coverage and costs resulting from Supreme Court decision (the framework is more important than the precise numbers) CBO projects that, by 2022*, based on Supreme Court decision: • 6 million fewer in Medicaid (growth of 11 million v. 17 million) • 3 million more with Exchange subsidies ( 20 million v. 17 million) • 3 million more uninsured (30 million v. 27 million) CBO projects federal spending changes from 2012-2022 period: • Medicaid down $288 billion • Exchange subsidies up $209 billion * Comparison of March, 2012 CBO update of impact of ACA with July 2012 Estimate updated for Supreme Court Decision. Note: CBO does not do State-by-State projections. Health Policy Alternatives 9-20-12
Key items in CBO projection • By 2022: • One-third of the potential new eligibles will be in States with full expansion up to 138% of FPL • One-half will be in states with partial expansion (up to 100% of FPL or lower – CBO assumes this option available in some form) • One-sixth of potential new eligibles will be in States that do not extend Medicaid • Phasing: of the newly covered Medicaid expansion population enrollees: • One-third will come in 2014 • One-third will come in 2015 • One-third will come in between 2016-2018 Health Policy Alternatives 9-20-12
Additional key items in CBO projection • Of the loss of 6 million in Medicaid coverage: • About 3/4 (about 4.5 million) are reductions in coverage of the newly eligible expansion population. • About 1/4 (about 1.5 million) are reductions in take-up by those already eligible for Medicaid or CHIP, who prior to the court decision were expected to enroll. That is, with fewer State expansions, awareness and take-up of current programs is expected to be lower. • For those with income between 100% - 138% of the FPL, take-up in Exchanges will be lower than take-up would have been in Medicaid (Exchange more attractive because it will offer better access, but less attractive because premiums and cost-sharing will be higher) • In general, federal cost of Exchange coverage about 50% higher than cost of Medicaid coverage ($9,000 v. $6,000) Health Policy Alternatives 9-20-12
Status of State Actions on Medicaid Expansion • No deadline for state decision in the ACA or set by CMS • Some governors (e.g., TX, FL, IA, LA, SC) have announced intention not to proceed with an expansion • Others have announced intention to do so (e.g., AR, MN, RI); • Legislatures may not agree • In most cases, expansion decision yet to be made (e.g., MO, VA, WI) Health Policy Alternatives 9-20-12
Essential Health Benefits Implementation • EHB Bulletin released December 16, 2011 http://cciio.cms.gov/resources/files/Files2/12162011/essential_health_benefits_bulletin.pdf • Frequently asked questions (2/17/2012) http://cciio.cms.gov/resources/files/Files2/02172012/ehb-faq-508.pdf • Actuarial value and cost-sharing reductions bulletin (2/24 /2012) http://cciio.cms.gov/resources/files/Files2/02242012/Av-csr-bulletin.pdf • Data collection to Support Standards Related to EHBs: Proposed Rule (6/5/2012) and Final Rule (7/20/2012) http://www.gpo.gov/fdsys/pkg/FR-2012-06-05/pdf/2012-13489.pdf http://www.gpo.gov/fdsys/pkg/FR-2012-07-20/pdf/2012-17831.pdf • State options for EHB benchmarks (7/3/2012) http://cciio.cms.gov/resources/files/largest-smgroup-products-7-2-2012.pdf.PDF • Notice of proposed rulemaking to be issued soon (?) Health Policy Alternatives 9-20-12
Proposed Benchmark Plan Types for 2014 and 2015 Department of Health and Human Services, CCIIO, Essential Health Benefits Bulletin. December 16, 2011, http://cciio.cms.gov/resources/files/Files2/12162011/essential_health_benefits_bulletin.pdf • States can select from four options for defining the benchmark plan • One of 3 largest small group insurance products in the state • One of 3 largest state employee plans in the state • One of the 3 largest FEHBP plan options • Largest HMO plan offered in state’s commercialmarket • Default if state does not make selection: largest product in state’s small group market • Definition of largest plans: enrollment data (first quarter of 2012 data used for 2014; rolling schedule for future years) • Deadline for state action is September 30, 2012 Health Policy Alternatives 9-20-12
Supplementing the Benchmark Plan • If benchmark plan does not include each of the 10 benefit categories, State must supplement: • Look first to largest plan in benchmark type selected by State that does offer the missing benefit • Then look to FEHBP • Considering options for likely gaps: habilitation, pediatric oral and vision care • For habilitation considering two options • Parity with rehabilitation • Plan decides, reports to HHS, with HHS deciding in future on benefit approach Health Policy Alternatives 9-20-12
EHBs and Benchmark Plans: State Options • 3 largest national FEHBP plan options • BCBS Standard (PPO) • BCBS Basic (PPO) • GEHA Standard (PPO) • 3 largest small group products in each state • Examples • CA – Kaiser, Anthem BC (1 HMO + 2 PPOs) • MD – two CareFirst, GHMSI (2 HMOs + 1 PPO) • OH – two Anthem plans and 1 Medical Mutual of Ohio (3 PPOs) • TX – two BCBS, UnitedHealthcare (2 PPOs+ 1 POS) CCIIO, Essential Health Benefits: List of the Largest Three Small Group Products by State, July 3, 2012 Health Policy Alternatives 9-20-12
7/20 EHB Data Submission Final Rule • Applies to issuers of 3 largest health insurance products, by enrollment, in small group market (March 31, 2012 data) • Applicable issuers to provide sufficient information so that issuers in individual and small group markets know what is included in the benchmark plans • Plan administrative data • All health benefits in the plan • Quantitative treatment limitations imposed on coverage • Eliminated proposed non quantitative limitations • Prescription drug coverage • Eliminated proposed collection of prior authorization and step therapy limits • Enrollment • Information to be submitted by issuers by 9/4/2012 Health Policy Alternatives 9-20-12
State Action on Benchmark Plans • 31 states have engaged in some formal activity around naming a benchmark plan (working group, review of state mandates, assessment of benchmarks, public comment) • CA: Legislation naming Kaiser small group HMO 30 plan as benchmark awaiting Gov. Brown signature • WA: Regence Innova Small Employer Plan plus gap-filling • 8 other states + DC have preliminary recommendations for benchmark plan (AR, CO, DC, NV, RI, UT, VA,VT,WA) • Of the states with benchmarks named or recommended, all but one are small group market plans; the other (UT) is a state employee plan Source: NASHP, http://www.statereforum.org/state-progress-on-essential-health-benefits Health Policy Alternatives 9-20-12
Other Anticipated Federal Standards • Quality reporting requirements for issuers and group health plans • 2014 insurance market reforms • Basic Health Plan standards • Employer and individual responsibility requirements • RFCs have been issued on discrete issues Health Policy Alternatives 9-20-12