Download
1 / 30
440 likes | 1.29k Views
Maastricht Classification of DCD. MC I, II, uncontrolled MC III, IV: controlled. An Introduction to Maastricht Category III DCD. Dr Paul Murphy National Lead for Organ Donation NHS Blood and Transplant, UK. Controlled DCD – the donation process. Objectives for the session – to understand.

E N D
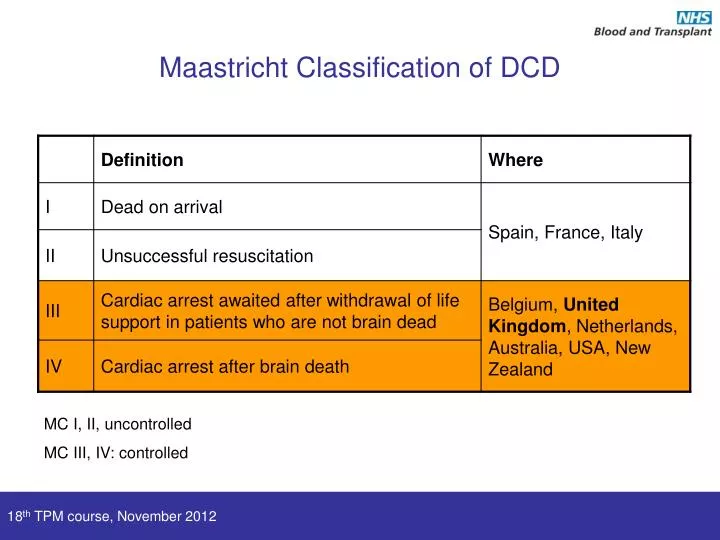
Maastricht Classification of DCD MC I, II, uncontrolled MC III, IV: controlled 18th TPM course, November 2012
An Introduction to Maastricht Category III DCD Dr Paul Murphy National Lead for Organ Donation NHS Blood and Transplant, UK 18th TPM course, November 2012
Controlled DCD – the donation process Objectives for the session – to understand • Definition of category III DCD • Key elements of the category III DCD pathway • Obstacles to DCD donation • Family approach and conflict of interest • Who can donate: prediction of asystole • Limitation of ischaemic injury • Diagnosis of death and post mortem interventions • Outcomes • Contribution to transplantation in UK 18th TPM course, November 2012
The pathway of controlled DCD The retrieval of organs from patients whose death is diagnosed on cardio-respiratory criteria and which follows the planned withdrawal of life-sustaining treatments. 18th TPM course, November 2012
How is end of life care changed to support DCD? 18th TPM course, November 2012
DCD as part of end of life care Key considerations • Donation considered before death • Withdrawal delayed by several hours • Physiological instability • Altered management of death • ? Withdrawal in anaesthetic room • Diagnosis of death after 5 minutes of asystole • Rapid transfer to theatre • Organ ischaemia and graft outcomes • Stand down • Substitution General overview We view DCD as part of the care we give patients when they die – offered, not imposed 18th TPM course, November 2012
DCD as part of end of life care Key considerations • Donation considered before death • Withdrawal delayed by several hours • Physiological instability • Altered management of death • ? Withdrawal in anaesthetic room • Diagnosis of death after 5 minutes of asystole • Rapid transfer to theatre • Organ ischaemia and graft outcomes • Stand down • Substitution General overview 40% of DCD retrievals in the UK are stood down. 18th TPM course, November 2012
Family approach and conflict of interest • Decision making around withdrawal of treatments should be transparent and consistent • All ICUs and EDs should have explicit local policies based upon national guidance • Multi-disciplinary • Donation should only be raised after a family have understood and accepted their loss • presented as an end of life care option “You should be prepared to follow any national procedures for identifying potential organ donors” GMC 18th TPM course, November 2012
Ischaemic injury in category III DCD decision re WLST cold perfusion transplant reperfusion withdrawal asystole cold ischaemia warm ischaemia terminal physiological decline SBP < 50mmHg SaO2 < 75% 18th TPM course, November 2012
Ischaemic injury decision re WLST cold perfusion transplant reperfusion withdrawal asystole agonal period cold ischaemia functional warm ischaemia SBP < 50mmHg SaO2 < 75% NB: timeline not to scale 18th TPM course, November 2012
Time to asystole • Younger age • High respiratory support • High FiO2 • PEEP > 10 cmH2O • IPPV • Inotropes • GCS 3 • Terminal extubation • BMI > 30 56% die within 60 mins 64% die within 2 hours 72% die within 4 hours Suntharalingam et al. AJT 2009;9:2157 18th TPM course, November 2012
40% DCD retrievals are stood down Practicality (agonal period) Ischaemic injury (functional warm ischaemia) Minimum agonal period is now 3 hours Current UK guidance on DCD stand down 18th TPM course, November 2012
t = 2 min Medical Centre University of Pittsburgh USA Solutions to ischaemic injury • Ante-mortem • Tissue typing and virological screening • Steroids, heparin, vasodilators • Femoral cannulation • Management at time of death • Withdrawal in theatre • Expedient diagnosis of death • Post-mortem reperfusion • In situ • Ex situ 18th TPM course, November 2012
Process of treatment withdrawal • Manner of treatment withdrawal should not be adjusted to promote donation • Complete withdrawal of all cardio-respiratory treatments • Inotropes • Ventilation • Endotracheal tube • Nursed in supine position • Pharmacological comfort cares as required 18th TPM course, November 2012
Location of treatment withdrawal 18th TPM course, November 2012
Diagnosis of Death In the UK, death can be confirmed after 5 minutes of complete and continuous absence of cardio-respiratory function………… www.aomrc.org.uk/publications/reports-guidance.html 18th TPM course, November 2012
Asystole is absence of mechanical cardiac function, not electrical silence on ECG It is best diagnosed by Invasive arterial pressure monitoring Echocardiography If invasive pressure monitoring or echocardiography are not available, identify on basis of isoelectric ECG Diagnosis of Death Death can be diagnosed after five minutes of continuous asystole 18th TPM course, November 2012
Death is confirmed by demonstrating the absence of neurological function (respiration, consciousness and brain-stem reflexes) after 5 minutes of continuous asystole Any return of cardiac or respiratory function must prompt further 5 minutes of observation Diagnosis of Death Death is regarded as the simultaneous and irreversible loss of consciousness and respiration 18th TPM course, November 2012
Diagnosis of death and organ retrieval • A clear intention not to perform cardio-pulmonary resuscitation • Confidence that the possibility of spontaneous return of cardiac function has passed • An absolute prohibition on any intervention that might restore cerebral oxygenation • Restoration of myocardial contractility • Extracorporeal oxygenation The brain remains responsive to restoration of oxygenation of some minutes 18th TPM course, November 2012
Methods of retrieval Perfusion in situ Intra-peritoneal cooling Crash laparotomy Super-rapid perfusion 18th TPM course, November 2012
Solutions to ischaemic injury Normothermic regional perfusion normothermic regional perfusion cold perfusion transplant reperfusion withdrawal asystole cold ischaemia Normothermic reperfusion serves to restore aerobic conditions prior to cold perfusion 18th TPM course, November 2012
Laparotomy, cannulation and perfusion with preservation solutions can begin as soon as death has been confirmed Regional normothermic perfusion of abdominal organs with oxygenated blood can take place as soon as the cerebral circulation has been isolated Reversing organ ischaemia 18th TPM course, November 2012
Re-intubation can take place as soon as death has been confirmed Lungs can be re-inflated with a single insufflation after 10 minutes Cyclical mechanical ventilation can only begin when the cerebral circulation has been isolated. Lung retrieval from DCD donors DCD donors may become the preferred source of lungs – particularly if assessed and re-conditioned ex-vivo 18th TPM course, November 2012
Deceased donation in UK, 2000-12 25% of DD transplants in the UK come from MC 3 DCD donors 18th TPM course, November 2012
Number of patients transplanted from UK deceased donors 1 April 2010 – 31 March 2011 25% of DD transplants in the UK come from MC 3 DCD donors 18th TPM course, November 2012
Cause of death in MC III DCD donors • UK Potential Donor Audit (October 2009 – March 2012) • 7504 patients referred as potential DCD donors • 877 actual DCD donors 18th TPM course, November 2012
DBD DCD UK kidney transplant outcomes for DBD/DCD donors Graft survival Patient survival 18th TPM course, November 2012
3 year patient survival 3 year transplant survival UK Liver transplant outcomes for DBD/DCD donors 18th TPM course, November 2012
3 year transplant survival UK Liver transplant outcomes for DBD/DCD donors 18th TPM course, November 2012
Summary • MC 3 DCD requires • modification to end of life care • organ retrieval to begin within minutes of diagnosis of death • considerable commitment from retrieval teams • There are anxieties over ischaemic injury • outcomes for kidney transplantation are acceptable • Interest in restoring circulation soon after death • MC 3 DCD accounts for almost all the increase in deceased donation in the UK over last 5 years 18th TPM course, November 2012