Download
1 / 27
270 likes | 415 Views
Letrozole versus hMG in intrauterine insemination cycles. H . Jamal; H. Serdaroglu; A. Baysoy; E. Karatekeli; E. Attar; H. Ozornek Istanbul, Turkey. Aromatase Inhibitors. i-Steroid group: Exemestane. ii-Non-Steroid imidazole group: Fadrozole.

E N D
Letrozole versus hMG in intrauterine insemination cycles H.Jamal; H. Serdaroglu; A. Baysoy; E. Karatekeli; E. Attar; H. Ozornek Istanbul, Turkey
Aromatase Inhibitors i-Steroid group: Exemestane ii-Non-Steroid imidazole group: Fadrozole. iii-Non-Steroid triazole group: Anastrazole, letrozole
letrozole letrozole reversible
Increases endogenous production of FSH Enhances ovarian response to gonadotropin stimulation Suppressing estrogen Increasing intraovarian androgen levels
Advantages of third-generation aromatase inhibitors • Extremely potent inhibition of aromatase • Very specific inhibition of aromatase without significant inhibition of other steroidogenesis enzymesOral administration100% bioavailability after oral administrationRapid clearance from the body (short half-life, ~ 45 hours) • No accumulation of the medications or their metabolites • No significant active metabolitesFew mild adverse effects with high tolerability when given chronicallyFew contraindications or drug interactionsRelatively inexpensive
Indications Breast cancer Endometrial cancer Endometriosis uterine fibroids a) Unexplained infertility b) PCO c) Poor responders Ovulation induction
IUI Human reproduction Mitwally et al. 2003 25 20 15 Clinical pregnancy rate 19.1% 10 18.7% 10.5% 5 0 FSH-only Letrozole- FSH CC-FSH
IUI Fertility and Sterility Healey et al. 2003 25 20 15 21.6% Clinical pregnancy rate 20.9% 10 5 0 FSH FSH+Letrozole
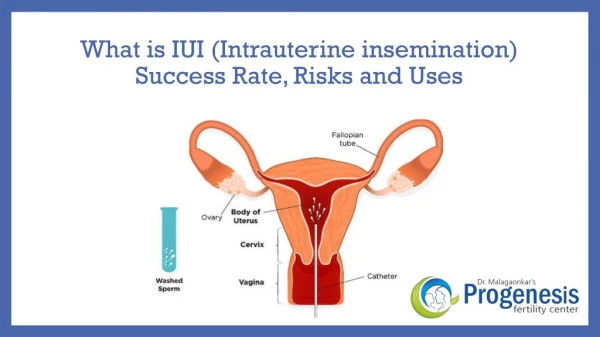
Objective A prospective randomized study comparing the results of intrauterine insemination (IUI) in women undergoing ovulation induction with either letrozole or Human Menopausal Gonadotropin (hMG).
IUI Letrozole group hMG group
80 couples regular menstrual cycles LETROZOLE GROUP(40 CASES) primary infertility female age <36 years hMG GROUP(40 CASES) All patients diagnosed as having unexplained infertility (lack of conception after at least 2 year of regular unprotected intercourse)
Transvaginal ultrasound • Hormone profiles • Semen analysis • Hysterosalpingogram • and/or Laparoscopy normal normal
OHSS and multiple pregnancy length of follicular phase clinical pregnancy rate endometrial thickness 14 mm follicles cost premature LH surge Letrozole & hMG
LH surge? LH-surge was defined as an increase in LH level ≥100% over mean of preceding two days.
HCG Letrozolevs hMG • Day 3 Day 7 • Day 3 Day 7 Letrozole 2x1 hMG 1x75ıu (<30 years) hMG hMG 1x150ıu(30years)
IUI was performed bythe same physician for all patients. No luteal support was given.
RESULTS Age (yrs) Duration of infertility (yrs) baseline FSH (IU/l) baseline LH (IU/l) baselin E2 (pg/ml) hMG (n=40) 28.1±4.3 5.9±3.2 6.11±1.7 5.29±2.1 41.74±13.4 Letrozole (n=40) 27.22±5.5 5.3±2.1 6.41±2.6 4.81±4.5 39.54±12.0 P: NS
RESULTS Semen parameters before preparation for insemination Letrozole [40] 31.43±4.1 63.9 ± 41.3 59.7 ± 16.1 52.9 ± 11.3 hMG [40] 30.10±5.9 66.3 ± 44.4 62.4 ± 15.3 54.1 ± 9.2 P value NS NS NS NS Age of male partner (yrs) Concentration (x106/ml) Motility (%) Normal sperm forms (%)
RESULTS hMG 11.90±1.7 3.21±1.6 10.05±2.9 95.6% 875.15±368 2 Letrozole 12.77±1.9 1.79±1.3 8.91±1.8 93.3% 193.19±80 2 P value NS <0.001 NS NS <0.001 NS Follicular phase(days) Follicle number Endometrial thickness(mm) Trilaminar pattern HCG day E2 Premature luteinization
RESULTS hMG 15 % 1(twin) 1(moderate) P value NS NS NS Letrozole 17.5% 1(triplet) 0 Pregnancy rate Multiple pregnancy OHSS
The mean dose of hMG (mean number of ampoules/cycle)was 15.5 ampoules/cycle. While the dose of letrozole were stable (10 tablets/cycle). Letrozole had a cost of 43 $ per cycle while hMG was more costly with 225 $ per cycle.
Conclusion • Although low estradiol levels and less number of mature follicles were obtained at the time of the hCG in the letrozole group, pregnancy rateswere similar in both groups.
Conclusion • Another outcome we noticed that the stimulation time lasted longer in the letrozole group. As other authors cited before that this longer time of stimulation may have beneficial effects on oocyte maturation and oocyte quality and this is maybe a reason that more pregnancies occured in the letrozole group.
Conclusion • Despite significantly lower E2 levels in the letrozole-treated women, endometrial development was unaffected, endometrial thickness and pattern were similar in both groups.
Conclusion • Serious complications (OHSS, multiple pregnancy) were rare in the two groups.Low estradiol levels and less number of mature follicles at the time of the hCG in the letrozole group may be a reason to minimize and thereby avoid the complications of ovarian hyperstimulation syndrome(OHSS) and multiple pregnancy. But to compare such an outcome, a large study including a very large number of patients must be required.
letrozole efficient cost effective simple and convenient