Download
1 / 37
440 likes | 1.32k Views
DISORDERS OF POTASSIUM HOMEOSTASIS. Informal Academic in Service. Overview. Hypokalemia Hyperkalemia Case Discussion. HYPOKALEMIA Serum potassium < 3.5 mEq /L. Pathophysiology. Total body potassium deficit Shifting of serum potassium into the intracellular compartment Causes

E N D
DISORDERS OF POTASSIUM HOMEOSTASIS Informal Academic in Service
Overview • Hypokalemia • Hyperkalemia • Case Discussion
Pathophysiology • Total body potassium deficit • Shifting of serum potassium into the intracellular compartment • Causes • Drugs (loop and thiazide diuretics) • Diarrhea • Vomiting • Hypomagnesemia
Principal cell Lumen Blood Na+ Na+ - + K+ K+ Aldosterone เพิ่มการดูดเกลือกลับขับ K+ออก Hypo Mg
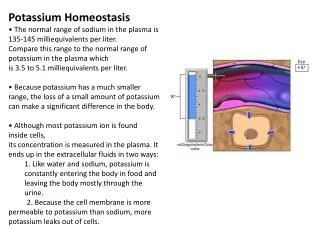
Principal cell Thaizide + Blood Lumen + Na+ - Na+ + - K+ + - K+ + ความต่างศักย์ไฟฟ้าคือ = 9 กรณีได้ HCTZ +
Principal cell Loop + Lumen Blood + - Na+ Na+ + - K+ - + K+ Ca2+ + Ca2+ ความต่างศักย์ไฟฟ้า คือ 3 กรณีได้ furosemide Ca2+ +
ดังนั้น HCTZ จึง lost K มากกว่า Furosemide
Clinical Presentation • Nonspecific signs and symptoms • Cardiovascular • Hypertension • Cardiac arrhythmias: heart block, atrial flutter, paroxysmal atrial tachycardia, ventricular fibrillation, and digitalis-induced arrhythmias • ECG effects (serum K <2.5 mEq/L): ST-segment depression or flattening, T-wave inversion and U-wave elevation • Neuromuscular symptoms • Muscle weakness, cramping, malaise and myalgias
Treatment • Every 1 mEq/L fall of K below 3.5 mEq/L Total body deficit of 100-400 mEq • Chronic used of loop or thiazide diuretics generally need 40-100 mEq of K K supplementation • Oral: KCl • IV: • severe hypokalemia • signs and symptoms of hypokalemia • Inability to tolerate oral therapy
Treatment K administration • Dilute in saline because dextrose can stimulate insulin secretion and worsen intracellular shifting of K • 10-20 mEq of K in 100 ml of NSS through a peripheral vein over 1 hr • ECG monitoring (If infusion rates > 10 mEq/hr)
Pathophysiology • Kintake > Kexcretion • Transcellulardistribution of K is disturbed Causes • Increased K intake • Decreased K excretion • Tubular unresponsiveness to aldosterone • Redistribution of K to the extracellular space • Drugs: ACEI, ARB, K-sparing diuretics
Clinical Presentation • Frequently asymptomatic • Heart palpitations or skipped heartbeats • ECG change (serum K 5.5-6 mEq/L) • Peaked T waves • Widening of the PR interval • Loss of the P wave • Widening of the QRS complex • Merging of the QRS complex with the T wave resulting in a sine-wave pattern
Treatment • Dialysis • Calcium administration • Insulin and dextrose, sodium bicarbonate, or albuterol • Sodium polystyrene sulfonate/Calcium polystyrene sulfonate
Treatment Dialysis • Most rapid lowering serum K Calcium • Rapidly reverses ECG & arrhythmias • Not lower serum K • Short acting • Must be repeated if signs or symptoms recur Insulin & dextrose/sodium bicarbonate/albuterol • Rapid shift potassium intracellularly
Treatment Sodium polystyrene sulfonate(kayexalate) • Mild to moderate hyperkalemia (K 5-7 mEq/L) • Each gram of resin exchanges 1 mEq of Na for 1 mEq of K • Sorbitol promotes excretion of K (by diarrhea) • Tolerated & effective: oral > rectal Calcium polystyrene sulfonate • Same kayexalate used • For patient who restriction of Na
Case 1 • ผู้ป่วยชายไทยอายุ 57 ปี • Supraventricular tachycardia, DM, HT • แพทย์ให้ Warfarin dose 15 mg/wk • ปรับเพิ่ม enalapril จาก 5 mg/day เป็น 10 mg/day • แพทย์ไม่ได้สั่ง spironolactone ต่อ consult ไม่พบแพทย์ • มียาเดิมเหลือ (spironolactone) จึงให้ทานยาเดิมก่อน • Advice sign of bleed/embolism • แพทย์นัด 12/01/54
LAB • INR 2.1 PT 22.7 • Hb 12.3 Hct 35.1 WBC 5360 Plate 229000 • Na 137 K 5.0 Cl 103 CO2 28 • BUN 22Cr 1.9 FBS 124
Subjective data • ผู้ป่วยชายไทยอายุ 57 ปี • Hx: Supraventricular tachycardia, DM, HT • Warfarin dose 15 mg/wk (dose เดิม) • แพทย์ปรับเพิ่ม enalapril จาก 5 mg/day เป็น 10 mg/day • แพทย์ไม่ได้สั่ง spironolactone และไม่ได้สั่ง off มียาเดิมเหลือ จึงให้รับประทานยาเดิมก่อน
Objective data • INR 2.1 PT 22.7 • K 5.0 • BUN 22Cr 1.9 • FBS 124 • แพทย์นัด 12/01/54
Assessment Spironolactone • Dose: 25-50 mg/day in 1-2 divide dose • Contraindication: hyperkalemia, acute renal insufficiency • ADR: gynecomastia, hyperkalemia, metabolic acidosis
Assessment Enalapril: • Dose: 2.5-5.0 mg/day then increase as require at 1-2 wk (Max 40 mg/day) • Contraindication: angioedema • ADR: hyperkalemia (1% to 3.8% )
Assessment • K 5.0 High potassium • Cr 1.9 mg/dl ClCr = 36 ml/min • Spironolactone ไม่แนะนำให้ใช้ถ้า ClCr < 10 ml/min • ดังนั้น จึงยังไม่จำเป็นต้องหยุด spironolactone Management • สามารถให้ยา enalapril ร่วมกับ spironolactone ต่อไปได้ • โดยติดตาม serum K, renal function และ ECG change
Plan Goal • Electrolyte balance Therapeutic plan • RM • Enalapril 5 mg 1x2 pc • Spironolactone 25 mg 1x1 pc
Plan Efficacy monitoring • K 3.5-5.0 mEq/L • BUN, Scr Toxicity monitoring • Hyperkalemia • Renal insufficiency
Plan Education plan • ติดตามอาการอ่อนเพลีย อัมพาต และ ภาวะการหายใจล้มเหลว • ใช้ยาตามที่แพทย์สั่ง Future plan • ติดตามการใช้ยาในครั้งต่อไป • ติดตามการเปลี่ยนแปลงของคลื่นหัวใจ
Case 2 • ผู้ป่วยหญิงไทย อายุ 47 ปี • มารับยาวาร์ฟารินตามแพทย์นัด • INR 2.37 • K 3.4 แพทย์สั่ง KCl elixir 10% ปริมาตร 15 ml PO stat
แพทย์สั่ง KCl elixir 10% 15 mlคิดว่า เหมาะสมหรือไม่?
Potassium Chloride • KCl 1 g ให้ Approximate K+ 13 mEq • 10% KCl elixir มี KCl 10 g/100 ml • ผู้ป่วยได้ 10% KCl elixir 15 ml = KCl 1.5 g • แสดงว่า ผู้ป่วยได้ K+ 19.5 mEq
Total K+ replecement • K+ 40 mEq oral เพิ่ม K+ในเลือด ~1 mEq/L • K+ 19.5 mEq oral เพิ่ม K+ในเลือด ~ 0.5 mEq/L • ดังนั้น คาดว่า จะเพิ่ม serum K = 3.4+0.5 = 3.9 mEq/L KNormal range = 3.5-5.0 mEq/L
References • Charles F Lacy, et al. Drug Information Handbook 2008-2009. 17th edition: 2008. • Barbara G Wells, et al. Pharmacotherapy Handbook. 7th edition: 2009. • สมาคมโรคเบาหวานแห่งประเทศไทยในพระราชูปถัมภ์สมเด็จพระเทพรัตนราชสุดาฯ สยามบรมราชกุมารี, สมาคมโรคต่อมไร้ท่อแห่งประเทศไทย สำนักงานหลักประกันสุขภาพแห่งชาติ. แนวทางเวชปฏิบัติสำหรับโรคเบาหวาน พ.ศ. ๒๕๕๑: 2552. • Mancia G, et al. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension. Journal of Hypertension: 25 (9), 2007. • http://www.thomsonhc.com