Download
1 / 33
330 likes | 661 Views
Autosomal Recessive Polycystic Kidney Disease (ARPKD) The disease with more than one face. Ihab Shaheen Consultant Paediatric Nephrologist RHSC- Glasgow. Learning objectives:. Epidemiology Genetics Clinical feature 2 Cases Differential diagnoses Prognosis Literature To take home.

E N D
Autosomal Recessive Polycystic Kidney Disease (ARPKD)The disease with more than one face Ihab Shaheen Consultant Paediatric Nephrologist RHSC- Glasgow
Learning objectives: • Epidemiology • Genetics • Clinical feature • 2 Cases • Differential diagnoses • Prognosis • Literature • To take home
Epidemiology: • Inherited disorder – progressive enlargement of renal collecting ducts varying degrees of hepatic abnormality • Rare 1:10,000 to 1:40,000 • Caucasians > other ethnic groups? • M = F
Epidemiology... • Estimated frequency of gene 1:70 in non isolated population • Incidence in isolated population 1:8000 ( Finnish) • Exact incidence is unknown: • Published studies vary in the cohort of cases examined • Some severely affected babies die perinatally without definite diagnosis
Genetics: • AR • Mutation in PKHD1, chromosome 6P21 • To date all kindereds with typical features of ARPKD have demonstrated linkage to this locus • Over 350 mutations have been recognized ( 2009)
Genetics... • Among the largest disease genes characterized to date in human genome (470 kb) • Encodes for polyductin/fibrocystin protein • This protein is localised in primary cilia mainly in the kidney • To lesser extent in liver, pancrease and arterial wall.
Genetics... • Genotype-phenotype correlation from type of mutation rather than the site of mutation • Truncating mutation displays severe form • Missense mutations are more frequent in less severe form
Clinical features: • Flank masses • HTN • Urinary concentration defect • Hyponatraemia • Renal insufficiency • Pulmonary hypoplasia • HSM • Oesophageal varices • hypersplenism
Renal: • Very rarely to be the cause of death in NN period • Usually improving following recovery from respiratory problems • Hyponatraemia is usually transient and related to the concentration defect • Fluid restriction could sort low Na but?
Hypertension • Unknown mechanism • 80% of affected children • ACE inhibitors,Ca channel blockers and beta blockers • Normal renin and aldosterone peripheral activity • May be related to local RAAS activation • Needs more than one agent to be controlled
Case 1.... • 35+3 premature Caucasian male • NVD, breech • Birth weight:2.3 kg • Normal antenatal scan • Both parents are under 30 • No F/H of renal diseases
Case 1... • Apgar of 1,9 @1 &5 minutes • 48 hrs of IV Ab • Needed initially CPAP, severe RD • Ventilated with surfactant x 2 • Right pneumothorax, needed chest drain
Case 1... • Generalised oedema by D2 • B/L large abdominal masses • Oliguria,low Na, high urea and creatinine • Urinalysis blood & protein +++ • Abdominal US: B/L PKD, most likely ARPKD, coarse liver.
Case 1... • Issues • Persistent HTN ( required 5 anti HTN& diuretics) • Poor weight gain • Renal failure • Family counselling
Case 2... • 8 year old female • Normal antenatal scan, no F/H of renal diseases • 38/40, NVD • RD, pneumothorax • Discovered to have ARPKD at the age of 4 months • Never needed dialysis
Case 2 ... • Kept on conservative treatment • Hypertension ( controlled by 2 anti HTN) • No concern regarding liver • Has LRD renal Tx from dad
Case 2 ... 3 months post renal Tx • Frequent blood Tx • Recurrent sepsis • Poor graft function • Massive spleenomegally
Case 2 ... Issues: • Graft nephrectomy • Haemodialysis • Combined liver-kidney Tx • Family disappointment
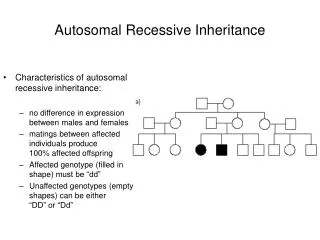
Diagnosis: • Diagnostic criteria were proposed by Zerresetal: • US features typical of ARPKD( enlarged,ecchogenic kidneys with poor CMD and • One or more of the following: a) absence of renal cysts in both parents particularly if they are > 30 years old
Diagnosis... b) clinical, lab or radiological evidence of hepatic fibrosis c) hepatic pathology demonstrating ductal plate abnormality d) previous affected sibling e) parental consanguinity suggestive of AR inheritance
Diagnosis... • Genetic testing is typically not required for patient with classic ARPKD • Prenatal diagnosis in a family with at least one affected child via mutation analysis • With identification and cloning of PKHD1, molecular analysis is now available
Neonatal large kidneys • Differential diagnosis includes - ARPKD - ADPKD - Glomerulocystic disease - Diffuse cystic dysplasia • Think about syndromes, e.g. Tuberous sclerosis , Zellweger syndrome Trisomy 13 ,etc…
Large NN kidneys • Other causes - RVT - Congenital NS - Contrast nephropathy - Renal candidiasis - Glycogen storage disease - Leukaemia
Clinical features of cystic diseases presenting in the newborn period
Clinical features suggesting ADPKD rather than ARPKD: • Positive F/H • Extrarenal cysts • Cerebral aneurysm • Asymptomatic presentation • Unilateral presentation • Haematuria • UTIs
Renal Cysts Unilateral disease Bilateral Disease Kidney size Parenchyma small and echogenic Large Normal or small Yes No Parents with ADPKD MCKD Simple cyst ,ADPKD, GCKD IVP demonstrates Pyramidal Blush Medullary Cysts Cortical Cyst Yes No Parents has Cystic Kidney disease ADPKD or GCKD Medullary sponge Kidney ADPKD Liver Disease Yes No Yes No MCD NPH ARPKD Consider ADPKD , NPH-type 2 and GCKD
Prognosis ARPKD • Improved with NNIC - 30% severely affected † NN period - for those surviving 1 yr survival 75-90% 5 yr survival 70-88% • Progression ESRF - > 50% - time variable • Common problems - feeding and growth failure - UTI - hepatic fibrosis - complications of RRT
Prognosis ARPKD... • Portal HT not uncommon • Significant risk for ascending bacterial cholangitis • Hepatic complications are the main reason of death in a 14 year follow up study post renal Tx
To take home • Significant phenotypic variability • Neonatal period - respiratory - fluid balance and electrolytes - hypertension • Prognosis improved with NNIC but progression to ESRF in >50%
To take home • Portal HTN can develop with normal synthetic liver function • Every patient with recurrent unexplained sepsis should be treated for cholangitis ( gram neg organisms) • Dietetic input is crucial • BP control could be a challenge