Download
1 / 13
320 likes | 1.02k Views
High Altitude Sickness. Terminology for High Altitude Sickness. AMS – acute mountain sickness Apnea – cessation of breathing Edema – local or systemic excesive accumulation of body fluids HACE – high altitude cerebral edema HAPE – high altitude pulmonary edeme

E N D
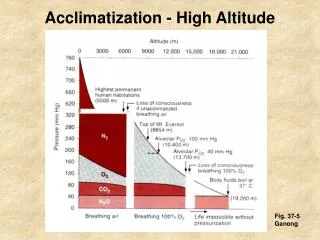
Terminology for High Altitude Sickness • AMS – acute mountain sickness • Apnea – cessation of breathing • Edema – local or systemic excesive accumulation of body fluids • HACE – high altitude cerebral edema • HAPE – high altitude pulmonary edeme • Hypobaric hypoxia – dec level of O2 in ambient air due to altitude
Altitudes greater than 10,00 feet place operators at risk • Sx listed as immediate and long term in exposure and display • Initial immediate response to altitude is hyperventilation triggered by hypoxia • Over a period of time the chemical stimulation causing hyperventilation will reverse – this may take from 10-14 days
60-80% of respiratory symptoms occur within 7-10 days of exposure • Acclimation to high altitude is effective in reducing this • Acclimation cannot be achieved in less than 10 days
Is your unit going above sea level? • Medical threat assessment for terrain • Paskistan army performs well above 4,000m due to prolonged acclimation • Acclimate your personnel as/when possible
Hyperventilation begins to alter the acid base balancee Decreased CO2 can seriously alter the effectiveness of the cardio vascular system Cellular walls begin to break down and fluid accumulation begins Initial Sx of headache occur for this increased intercranial pressure related headache Recognition of this early onset Sx and descending will abate serious condition later Progression
Despite Acclimation Sx may still occur • Sx vary from mild to life threat • All are mission limiting for the soldier and cannot be ignored • HAPE & HACE are life threats without ALS intervention
Risk Factors • Degree of acclimation • Ascent rate • Height achieved • Altitude soldier sleeps at • *Fitness level of soldier population is not commonly a protective measure ensuring protection from Altitude Sickness
Initial Presentation of Acute Mountain Sickness (AMS) • Headache in a recently arrived person at altitudes greater than 2500m • GI distress common • Insominia, dizziness, fatigue is the progression
HACE / HAPE • Clinical Dx made after severe symptoms to include respiratory distress and marked decreased level of consciousness • Evidence of retinal hemorrhage is evidentiary to above • Drowsiness to stupor is a common patient presentation
Management • Stop further ascent • Descend as soon as practical at 1st signs of severe symptoms
Somestimes descending a few hundred meters is enough to reverse symptoms Use of a portable HBO chamber will improve the condition 2 PSI over ambient will simulate a 2500m drop in altitude Medical Therapy
Summary • Medical threat assessment when about to operate above 2500 m • Acclimate early • Expose slowly over a period of 2wks • Descend or seek ALS before Sxs progress • Mild AMS can still affect mission effectiveness • HACE/HAPE are life threats descend!