Download
1 / 54
901 likes | 1.97k Views
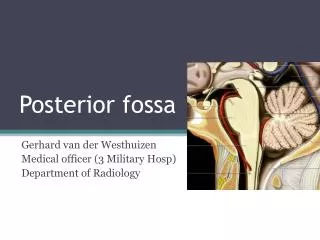
Anaesthetic considerations in posterior fossa surgery . Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics PhD ( physio ) Mahatma Gandhi medical college and research institute , puducherry – India . What is it ??. Boundaries :.

E N D
Anaesthetic considerations in posterior fossa surgery Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio)Mahatma Gandhi medical college and research institute , puducherry – India
Boundaries : • Anteriorly : clivus, petrous part of temporal bone • Posteriorly: occipital bone • Laterally : squamous and mastoid part of the temporal bone • Superiorly : tentoriumcerebelli • Inferiorly : Foramen magnum
Why do we specially care about this ?? • brainstem, • The cerebellum • fourth ventricle. • What is in brainstem??
The Respiratory center; • The Cardiovascular center; • The Swallowing center; • The Center of vomiting, coughing, • and/or hiccups; • The Chewing center; • The Salivary centers. • The Brainstem Reticular Substance
The cerebellum • coordination, controlling voluntary and involuntary motor activity like balance and locomotion alcoholic ?? cranial nerve nuclei Flow of CSF
Tumours • Young – primary tumours and aneurysms • Medulloblastomas, ependymomas, gliomaastrocytomasglomusjugulare tumors • ( Pneumonic - MEGA – GA ) • Old age -- ?? Secondary lesions
Presentation • ICH - herniation , ischemia • Movement disorders • Cerebellum • Autonomic disturbance • Cranial nerve disorders
Preanaesthetic concerns • Routine • + + + + • Cardiovascular status – is he/she fit for sitting position ?? • Altered sensorium • Cranial nerve palsies, aspiration pulmonary infection • Debilitation and nutrition • Diuretics and electrolytes
Preanaesthetic concerns • Discussion with surgeon for invasive monitors • Preoperative audiometry is useful in predicting hearing preservation after acoustic shwannoma surgery • Residual motor, sensory deficits, speech deficits recorded
Preop evaluation • Obtain the results of any recent intracranial or diagnostic procedure and consider possibility of residual pneumocephalus . prev. surgeries • Drug history • Steroid, mannitol, antihypertensive, tricyclic antidepressants ,L –dopa, benzodiazepines, phenothiazines ,
Anaesthetic considerations • Premed • Benzodiaepines • Antisialogogues • May avoid narcotics
Transfer • Given the value of a head-up posture for controlling ICP, it is recommended that patients with mass lesions be transported with the head of the bed elevated 15–30°.
Goals in anaesthesia • to facilitate surgical access, • minimize nervous tissue trauma and maintain respiratory and cardiovascular stability,(cranial nerves ) VAE prevention and identification • CPP , ICP, CMRo2 – comes next in posterior fossa surgery
Prone position nipple genital Minimal neck flexion anterior flexion, abducted and externally rotated No pressure in axilla Abdomen free Face in soft headring with no pressure on eyes and nose Elbow padded
Sitting • Not frequently used • Craniotomy • Good surgical access, CSF drainage, easy airway access • Venous return decrease and cardiac output decrease • HR no change • Venous air embolism
Contraindications for sitting position • Intracardiac defects • Unstable hemodynamics • Cachexia • Severe hydrocephalus • extremes of age • Degenerative diseases of cervical spine • Significant CVD.
Lateral Or Park Bench Position • Can be used for access to the post parietal & occipital lobes & lat. post fossa, including tumors at the cerebellopntine angle & aneurysms of the vertebral & basilar arteries.
Monitoring • The goals of monitoring are to ensure adequate CNS perfusion maintain cardiovascular stability and detect and treat VAE ( venous air embolism ) • Five lead ECG, Pulse oximetry, NIBP, IBP • EtCO2 monitoring • Temperature • Central venous catheter • Precordialdoppler probe FOR VAE • Esophageal stethoscope • TEE
What is special • diuresis, blood glucose, hematocrit. • Electromyography • ICP -- ??? • SSEP, • MEP ( cranial nerves especially 7 )
Special • Facial nerve - CP angle tumours – muscle relaxant use to be restricted • SSEP – integrity of neural tracts , tension pneumocephalus , spinal cord ischemia • Evoked potential – agents • BERA – less sensitive to agents – glomusjugulare
Anaesthetic technique • Induction of anesthesia is a critical time • Hypotension, hypertension bradycardia, cough • Templehoff's scale – choice of agent and technique
Templehoff's scale • Easy use; • • Rapid induction and awakening; • • Maintenance of perfusion and self-regulation; • • Prevention of ICP rise • • Maintenance of vascular reactivity to CO2; • • Lack of systemic toxicity; • • Possibility of electrophysiological monitoring; • • Low cost.
Painful times • Laryngoscopy, tracheal intubation; • • Fixing the head in the headrest; • • Skin, periosteum, and dura matter • incision • • Suture of dura matter and scalp.
TIVA • Explanation • Fentanyl - 1 – 2 mic / Kg • Midazolam 1 mg IV • Propofol - 1.5 – 2 mg / kg ( 0.1 mg /kg/hour) • TCI of 3 – 4.4 mic gm / ml • With or without relaxants , • Local infiltration • ANY WAY – INTUBATE
Pros and cons – TIVA • Monitoring !! • CBF reduced • Recovery • Awareness • Increased complications
Balanced GA technique 1) Preoxygenation and self hyperventilation 2.) Thiopentone 3-4 mg/kg IV. 3.) Vecuronium 0.1 mg/kg IV and mask hyperventilation with oxygen and N2O (50:50) until neuromuscular blockade achieved. ISO CAN BE ADDED 4.) Lidocaine 1.5 mg/kg IV and additional thiopentone 2 mg/kg IV just before ET Intubation.
Others • Rapid sequence is an alternative • Maintenance : • 1. Fentanyl 5 mic /kg with 0.5 % iso • 2.Fentanyl 1.5 mic /kg with 1.5 % iso • Isoflurane – mild cerebral vasodilation and less effect on autoregulation
RELAXANTS • Muscle relaxation is also important during neurosurgery relaxation prevent patient movement at inappropriate time • it may decrease ICP by relaxing the chest wall with decrease intra thoracic pressure and encourage venous drainage. • Vecuronium – no effect on brain – BUT phenytoin
FLUIDS Dry but stable patient is optimum for tumor surgery. • Preferably no dextrose • Tube fixation – extra care • Spontaneous breathing –respiratory structures
Emergence • It should be smooth and gentle. • Lidocaine 1.5 mg/kg IV decrease cough and strain. • If surgery is superficial and performed without much traction on the brain stem,-- may extubate. • If lesion is deep seated with frequent traction on the brain stem there may be danger of apnea or decrease sensorium with diminish airway reflexes,- keep ventilating - awaken slowly
Points to ponder before extubation • Level of consciousness • Airway and gag reflex • Face and tongue edema • Airway edema • Regular respiratory pattern • Stable vital parameters
Intraoperative • Arrhythmias • Ventricular and supraventricular arrhythmias can occur from brain stem stimulation.
CVS side effects • Hypertension results from stimulation of V th CN, periventricular gray area, reticular formation, or nucleus of tractussolitarius. • Bradycardia and escape rhythms results from vagus N stimulation, • Hypotension can results from pontine or medullary compression.
Venous Air Embolism • 25 – 50 % in sitting position • That dose not mean it cant happen in other positions
Causes open veins & non collapsible venous channels gravitational effects of low CVP neg. I.v. pressure relative to atm. Pressure poor surgical technique
Treatment • Notify the surgeon to flood the surgical site • Lower the operative site • Stop N2O administration • Give 100% O2 • Perform aspiration through a central venous line • Consider compression of the jugular veins • Provide cardiopulmonary support (fluids, pressors, inotropes)
Pneumocephalus • Air into the epidural or dural space sufficient to exert a mass effect. • Incidence- 3% • Sometimes life threatening brain herniation.
CAUSES: • Diminution of brain volume mannitol, hyperventilation, removal of SOL • contraction of intravascular blood vol. associated with acute hemorrhage • Gravitational effect of sitting position • Intraop drainage of CSF • “Inverted Pop Bottle Analogy” as CSF pours out, air bubbles to the top of the container(cranium)
Clinical features • Confusion • Headache • Convulsions • Neurological deficits • Failure to regain conciousness
Diagnosis and treatment CT scan confirms the diagnosis and localisation of intracranial air, if untreated Brain herniation and death. Treatment • IMMEDIATE twist drill aspiration of air through burr holes on either side of the vertex. • Nitrous ??
Hydrocephalus • Hydrocephalus – CSF obstruction at the level of fourth ventricle
MACROGLOSSIA • Extreme flexion of head with chin resting on the chest • Prolong presence of an oral airway Obstruction of its venous and lymphatic drainage Airway obstruction postop hypoxemia, hypercapnia