Download
1 / 25
260 likes | 1.22k Views
Basic Science. Venturi effectBernoulli principleturbulence ? stridor. Basic Science. glottissupraglotticsubglotticintrathoracic trachea. Basic Science. pedi airway narrowest at subglottiscross-section of airway proportional to square of radius (?r2). Supraglottitis. ?angina epiglottidea anterior"bacterial cellulitis of supraglottis2 to 7 years oldHaemophilus influenzae type B most commonincidence greatly decreased since vaccine.

E N D
1. EPIGLOTTITIS, CROUP AND TRACHEITIS Robert H. Stroud, M.D.
Norman R. Friedman, M.D.
10 March 1999 Acute infections of airway common in pediatric population
leading cause of hospital admission of children less than 4
mild, self-limited dz that may never be seen by MD, to potentially life-threatening
diagnosis often on PE, radiology for case atypical
airway protection always foremost when evaluatingAcute infections of airway common in pediatric population
leading cause of hospital admission of children less than 4
mild, self-limited dz that may never be seen by MD, to potentially life-threatening
diagnosis often on PE, radiology for case atypical
airway protection always foremost when evaluating
2. Basic Science Venturi effect
Bernoulli principle
turbulence � stridor Stridor is sign not diagnosis (diff dx slide)
normally approx laminar flow, inflammation leads to narrowing
Venturi effect (Venturi/Bernoulli slide)
Bernoulli principle
turbulence manifest as stridorStridor is sign not diagnosis (diff dx slide)
normally approx laminar flow, inflammation leads to narrowing
Venturi effect (Venturi/Bernoulli slide)
Bernoulli principle
turbulence manifest as stridor
3. Basic Science glottis
supraglottic
subglottic
intrathoracic trachea Glottic obs-inspiratory early, biphasic late - cartilage framework
supraglottis - inspiratory, soft tissue collapse with negative pressure
distal and subglottic narrowing increased with positive intrathoracic pressure during exhalation - expiratory stridor or wheezing
Glottic obs-inspiratory early, biphasic late - cartilage framework
supraglottis - inspiratory, soft tissue collapse with negative pressure
distal and subglottic narrowing increased with positive intrathoracic pressure during exhalation - expiratory stridor or wheezing
4. Basic Science pedi airway narrowest at subglottis
cross-section of airway proportional to square of radius (?r2) Adult and pedi airway different, children more susceptible
subglottis narrowest
rigid cricoid with loose submucosa
pi r squared/ pi r squared = r2/r2 (6mm, 1 mm edema = 44% narrowing)
worse with subglottic stenosis
Adult and pedi airway different, children more susceptible
subglottis narrowest
rigid cricoid with loose submucosa
pi r squared/ pi r squared = r2/r2 (6mm, 1 mm edema = 44% narrowing)
worse with subglottic stenosis
5. Supraglottitis �angina epiglottidea anterior�
bacterial cellulitis of supraglottis
2 to 7 years old
Haemophilus influenzae type B most common
incidence greatly decreased since vaccine Michel 1878
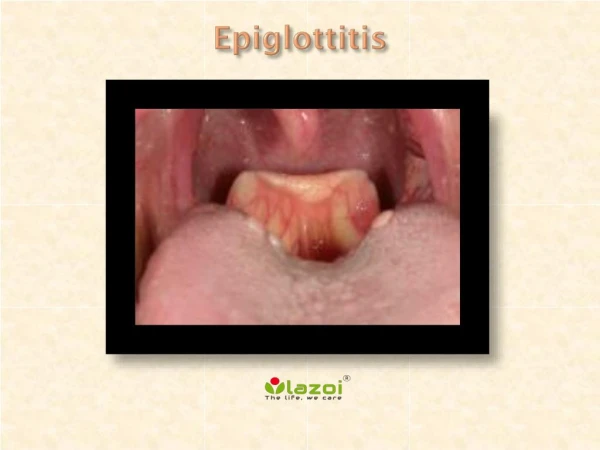
involves all supraglottic structures including epiglottis (lingual surface), AE folds, arytenoids
epiglottis pushed post - progressive airway obs
2-7 yo, occ less than 1yo
HIB most common, group A beta hemolytic strep, staph, pneumococcus, kleb, pseudomonas, candida, viruses
HIB vaccine mid-1980�s - huge decrease in incidence 3.47/100,000 to 0.63
organisms beside HIB more commonMichel 1878
involves all supraglottic structures including epiglottis (lingual surface), AE folds, arytenoids
epiglottis pushed post - progressive airway obs
2-7 yo, occ less than 1yo
HIB most common, group A beta hemolytic strep, staph, pneumococcus, kleb, pseudomonas, candida, viruses
HIB vaccine mid-1980�s - huge decrease in incidence 3.47/100,000 to 0.63
organisms beside HIB more common
6. Supraglottitis odynophagia
fever
irritability
stridor
rapidly progressive Acute onset fever, throat pain, irritability, respiratory distress (stridor late)
rapidly progressive (hours)
toxic, sitting, leaning forward - +/- drooling, muffled voice, limited speech
secondary infection in 50% - meningitis, OM, pneumonia
Acute onset fever, throat pain, irritability, respiratory distress (stridor late)
rapidly progressive (hours)
toxic, sitting, leaning forward - +/- drooling, muffled voice, limited speech
secondary infection in 50% - meningitis, OM, pneumonia
7. Supraglottitis if suspected, diagnose by direct laryngoscopy in OR
lateral neck film - �thumb sign�
1nasotracheal intubation
IV antibiotics
extubate when air leak noted - usually within 48 hours If hx and PE consistent - to OR for DL for diagnosis
MD capable of airway control with pt at all times
no intraoral exam, phlebotomy or other procedures that may upset child
sit in parents lap
x-rays if ? Dx and no resp distress - lat neck with thumb sign and hypopharyngeal over distention (loss of vallecular air space, thick epiglottis and AE folds)
normal subglottis on AP
Endoscopy as quickly as possible - always accompany pt
communication b/t endoscopist and anesthesiologist spontaneous ventilation - orotracheal intubate (anesthesia or Oto)
rigid telescope with ETT threaded over it, brochoscopes (age approppriate and size smaller), trach set-up
draw blood after airway secure - CBC and cultures
thorough endoscopy with cultures
NT intubation, IV abx (Amp/Chlor, Ceftriaxone, Cefuroxime, Unasyn)
If hx and PE consistent - to OR for DL for diagnosis
MD capable of airway control with pt at all times
no intraoral exam, phlebotomy or other procedures that may upset child
sit in parents lap
x-rays if ? Dx and no resp distress - lat neck with thumb sign and hypopharyngeal over distention (loss of vallecular air space, thick epiglottis and AE folds)
normal subglottis on AP
Endoscopy as quickly as possible - always accompany pt
communication b/t endoscopist and anesthesiologist spontaneous ventilation - orotracheal intubate (anesthesia or Oto)
rigid telescope with ETT threaded over it, brochoscopes (age approppriate and size smaller), trach set-up
draw blood after airway secure - CBC and cultures
thorough endoscopy with cultures
NT intubation, IV abx (Amp/Chlor, Ceftriaxone, Cefuroxime, Unasyn)
8. Laryngotracheobronchitis croup - Scottish for barking cough
6 months to 3 years old
Parainfluenza viruses types 1 and 2 most common Croup - Scottish, barking cough with many airway congenital and infectious airway lesions
LTB most appropriate
6 month to 3 yrs
under 1 yr - ? Subglottic stenosis
90% of acute airway obs, 3-5% of all children have one episode, 5% recurrent, hospitalization rare, intubation very rare 1-5%
Parainfluenza viruses 1&2, influenza A&B, RSV, HSV I, measles, adenovirus and varicella all reported
Croup - Scottish, barking cough with many airway congenital and infectious airway lesions
LTB most appropriate
6 month to 3 yrs
under 1 yr - ? Subglottic stenosis
90% of acute airway obs, 3-5% of all children have one episode, 5% recurrent, hospitalization rare, intubation very rare 1-5%
Parainfluenza viruses 1&2, influenza A&B, RSV, HSV I, measles, adenovirus and varicella all reported
9. Laryngotracheobronchitis URI symptoms
barking cough
hoarseness
inspiratory stridor
low-grade fever URI for several days
barking cough, low-grade fever, hoarseness, stridor (inspiratory, biphasic severe)
Croup scores - several - Westley most commonly used- not practical
stridor
air entry
level of consciousness
cyanosis
retractions
URI for several days
barking cough, low-grade fever, hoarseness, stridor (inspiratory, biphasic severe)
Croup scores - several - Westley most commonly used- not practical
stridor
air entry
level of consciousness
cyanosis
retractions
10. Laryngotracheobronchitis laryngoscopy for those with respiratory distress
AP neck - �steeple sign�
supraglottis normal AP neck - steeple sign, normal supraglottis
dynamic obs, increased on inspiration, subglottic stenosis and hemangiaoma fixed with resp cycle
Expiratory film useful to differentiate fixed from dynamic obstruction
widening of stenosis on expiration:
unilat VF paralysis
LTB
no change:
subglottic stenosis
bacterial tracheitis
normal x-rays in 50%
flexible fiberoptic exam OK if pt coop and no distress
OR for severe distressAP neck - steeple sign, normal supraglottis
dynamic obs, increased on inspiration, subglottic stenosis and hemangiaoma fixed with resp cycle
Expiratory film useful to differentiate fixed from dynamic obstruction
widening of stenosis on expiration:
unilat VF paralysis
LTB
no change:
subglottic stenosis
bacterial tracheitis
normal x-rays in 50%
flexible fiberoptic exam OK if pt coop and no distress
OR for severe distress
11. Laryngotracheobronchitis usually self-limited
humidified air
racemic epinephrine
steroids
heliox
intubation for severe, refractory cases Usu self limited, most do not seek medical attention
humidified air - no studies to prove benefit, strong anecdotal evidence - soothe mucosa, moisten secretions for easier expectoration
racemic epi - vasoconstrictive - l-rotatory cheaper and same benefit, improve in 10-30 minutes, lasts 2 hours, REBOUND - ? Need for hospitalization - obs 3 hours
steroids - ? Action - decrease perm of cap endothelium, stabilize lysosomal membranes - decrease inflammatory cascade and submucosal edema - 3 hours to onset of effect
used since 60�s - Klassen and Johnson (decreased hosp rate as compared to placebo), nebulized Budesonide not available in US, no clear benefit and more expensive
Dexamethasone 0.6 mg/kg/day po/IM/IV, Prednisolone 2.0 mg/kg/day divided or Dexamethasone 1.0 mg/kg/day divided
heliox - promotes laminar flow, deceased work of breathing
endoscopy if unresponsive, NT intubation, small tube, extubate in several days after airleak, scope for recurrent, atypical (5-7 day intubation), unresponsive, youngUsu self limited, most do not seek medical attention
humidified air - no studies to prove benefit, strong anecdotal evidence - soothe mucosa, moisten secretions for easier expectoration
racemic epi - vasoconstrictive - l-rotatory cheaper and same benefit, improve in 10-30 minutes, lasts 2 hours, REBOUND - ? Need for hospitalization - obs 3 hours
steroids - ? Action - decrease perm of cap endothelium, stabilize lysosomal membranes - decrease inflammatory cascade and submucosal edema - 3 hours to onset of effect
used since 60�s - Klassen and Johnson (decreased hosp rate as compared to placebo), nebulized Budesonide not available in US, no clear benefit and more expensive
Dexamethasone 0.6 mg/kg/day po/IM/IV, Prednisolone 2.0 mg/kg/day divided or Dexamethasone 1.0 mg/kg/day divided
heliox - promotes laminar flow, deceased work of breathing
endoscopy if unresponsive, NT intubation, small tube, extubate in several days after airleak, scope for recurrent, atypical (5-7 day intubation), unresponsive, young
12. Spasmodic Croup presentation similar to LTB
sudden onset stridor
afebrile
recurrent episodes that resolve spontaneously
unknown cause barking cough, stridor, sudden onset usually at night
afebrile without URI sx�s
often recurrent and reslove spontaneously
unknown pathogenesisbarking cough, stridor, sudden onset usually at night
afebrile without URI sx�s
often recurrent and reslove spontaneously
unknown pathogenesis
13. Bacterial Tracheitis Jackson - 1945, Jones - 1979
6 months to 8 years old
bacterial infection complicating viral LTB
Staph aureus most common described as early as 1945 by Jackson but Jones in 1979 detailed description
bacterial LTB, membranous LTB, pseudomembranous croup
rare but should be included in diff dx of resp distress as may be life-threatening
6 months to 8 yesrs
complication of LTB, bacterial superinfection
Staph most common, Moraxella in recent study by Bernstein et al, HIB, Strep
described as early as 1945 by Jackson but Jones in 1979 detailed description
bacterial LTB, membranous LTB, pseudomembranous croup
rare but should be included in diff dx of resp distress as may be life-threatening
6 months to 8 yesrs
complication of LTB, bacterial superinfection
Staph most common, Moraxella in recent study by Bernstein et al, HIB, Strep
14. Bacterial Tracheitis URI symptoms
acute onset high fever and respiratory distress
no odynophagia similar to LTB with URI sx, then acute onset high fever, resp distress, toxic
no drooling or odynophagia
increased WBC count, may have secondary infection, pneumonia common
similar to LTB with URI sx, then acute onset high fever, resp distress, toxic
no drooling or odynophagia
increased WBC count, may have secondary infection, pneumonia common
15. Bacterial Tracheitis �steeple sign� on AP neck
intraluminal soft tissue irregularities
endoscopy best diagnostic method to OR for those in resp distress
�steeple sign�
hazy tracheal air column with scalloping due to pseudomembrane detachment
endoscopy diagnostic method of choice to OR for those in resp distress
�steeple sign�
hazy tracheal air column with scalloping due to pseudomembrane detachment
endoscopy diagnostic method of choice
16. Bacterial Tracheitis subglottic edema
ulceration
pseudomembrane formation
suction and debride
nasotracheal intubation
IV antibiotics
extubate after 3-7 days endoscopy with spontaneous ventilatin
glottic and subglottic edema, ulceration and pseudomembrane formation in trachea
purulent materail and sloughed mucosa
suction and debride with FB forceps
Gram stain, culture and sensitivites
decision for intubation made case-by-case, 57% in study by Bernstien but 80% historically
3-7 days, extubate when fever down and secretion s down
anitbiotics for Staph - nafcillin + Ceftriaxone, Cefuroxime, Unasyn OK
14 day of abx (IV and oral)endoscopy with spontaneous ventilatin
glottic and subglottic edema, ulceration and pseudomembrane formation in trachea
purulent materail and sloughed mucosa
suction and debride with FB forceps
Gram stain, culture and sensitivites
decision for intubation made case-by-case, 57% in study by Bernstien but 80% historically
3-7 days, extubate when fever down and secretion s down
anitbiotics for Staph - nafcillin + Ceftriaxone, Cefuroxime, Unasyn OK
14 day of abx (IV and oral)
17. Case Study 1 14 month old male
breathing difficulties
2-3 days of URI symptoms
this morning, cough and loud breathing sound Is this stridor? Age at onset - today
Duration - hours
Position - no association
Assoc sx - feeding - OK
cyanosis - none
agitation - none
Cough description - any choking episode?
Dry or productive?
More in AM or at night?
Any prior episodes? 2 - 4 & 8 months of age, took one week to improve
Social - Daycare, Home, Immunizations
Is this stridor? Age at onset - today
Duration - hours
Position - no association
Assoc sx - feeding - OK
cyanosis - none
agitation - none
Cough description - any choking episode?
Dry or productive?
More in AM or at night?
Any prior episodes? 2 - 4 & 8 months of age, took one week to improve
Social - Daycare, Home, Immunizations
18. Case Study 1 afebrile, respirations 26/min, pulse 124 beats/min
reclining in mother�s lap, NAD
soft, biphasic stridor
lungs clear to auscultation VS normal for age, sitting quietly in mother�s lap
soft, musical biphasic stridor
volume - loud more severe obstruction
sudden decrease may indicate near complete obs
Pitch - low: nose, NP, supraglottis
high: glottis
intermediate: subglottis
Phase - inspiratory: supraglottic
expiratory: intrathoracic
biphasic: glottic or subglotticVS normal for age, sitting quietly in mother�s lap
soft, musical biphasic stridor
volume - loud more severe obstruction
sudden decrease may indicate near complete obs
Pitch - low: nose, NP, supraglottis
high: glottis
intermediate: subglottis
Phase - inspiratory: supraglottic
expiratory: intrathoracic
biphasic: glottic or subglottic
19. Case Study 1 laryngotracheobronchitis
differential: epiglottitis, bacterial tracheitis, foreign body, subglottic stenosis
20. Case Study 1 lateral airway film - neck extended, inspiratory
racemic epinephrine
oral dexamethasone Lateral airway film all that is needed - inspiratory with neck extended - hypopharynx filled with air
Expiratory film useful to differentiate fixed from dynamic obstruction
widening of stenosis on expiration:
unilat VF paralysis
LTB
no change:
subglottic stenosis
bacterial tracheitis
Labs: CBC and cultures
racemic epinephrine
dexamethasoneLateral airway film all that is needed - inspiratory with neck extended - hypopharynx filled with air
Expiratory film useful to differentiate fixed from dynamic obstruction
widening of stenosis on expiration:
unilat VF paralysis
LTB
no change:
subglottic stenosis
bacterial tracheitis
Labs: CBC and cultures
racemic epinephrine
dexamethasone
21. Case Study 1 observe for 3 hours
vastly improved at 4 hours post-treatment
consider direct laryngoscopy and bronchoscopy in 3-4 weeks discharge or admission - obs 3 hours,
vastly improved at 4 hours
?mitigating circimstances
follow-up - repeat airway films
DL and B for early onset and recurrence (3-4 weeks)
discharge or admission - obs 3 hours,
vastly improved at 4 hours
?mitigating circimstances
follow-up - repeat airway films
DL and B for early onset and recurrence (3-4 weeks)
22. Case Study 2 6 year old
rhinorrhea, cough, low grade fever
acute onset high fever and stridor several days URI, rhinorrhea, low grade temp
ED with acute onset high fever and resp distress (102.7)
o2 sat 95-97% on RA
retraction and harsh barking cough
several days URI, rhinorrhea, low grade temp
ED with acute onset high fever and resp distress (102.7)
o2 sat 95-97% on RA
retraction and harsh barking cough
23. Case Study 2 to OR for endoscopy
edematous larynx
ulceration and sloughing of tracheal mucosa
purulent secretions in right lower lobe 5.0 mm tube by anesthesia
CBC with WBC 19000
glottic edema, ulceration with purulent material in trachea - cleaned
5.0 mm tube by anesthesia
CBC with WBC 19000
glottic edema, ulceration with purulent material in trachea - cleaned
24. Case Study 2 nasotracheal intubation
IV Cefuroxime
S. aureus
CXR with right lower lobe pneumonia
extubated 4th day post intubation NT intubation
IV Cefuronxime
RLL pneumonia by CXR
cx S. aureua sens to Cefuroxime
clinically imporved and extubated in 4th day after intubation after leak with positive pressure
d/c�d 7 days after admission on po abx for total of 14 days therapyNT intubation
IV Cefuronxime
RLL pneumonia by CXR
cx S. aureua sens to Cefuroxime
clinically imporved and extubated in 4th day after intubation after leak with positive pressure
d/c�d 7 days after admission on po abx for total of 14 days therapy
25. Controversies and Future drastic decrease in supraglottitis as a result of vaccine
nasotracheal intubation for supraglottitis
disposition of children treated for LTB with epinephrine
steroids in LTB HIB vaccine - incidence deceased (Bailey 3.47 cases per 100,000 in1980to 0.63 in 1990
incidence in adults stable
other organisms besides HIB more common
airway in supraglottitis - now NT intubation, past trach - ? obs in ICU
LTB - disposition in pts treated with epi - admit or home after obs for a few hours
steroids - Dexamethasone - dose and route of administration
nebulized Budesonide - ? any benefit
who should receive it? nedd clear cut indicators
HIB vaccine - incidence deceased (Bailey 3.47 cases per 100,000 in1980to 0.63 in 1990
incidence in adults stable
other organisms besides HIB more common
airway in supraglottitis - now NT intubation, past trach - ? obs in ICU
LTB - disposition in pts treated with epi - admit or home after obs for a few hours
steroids - Dexamethasone - dose and route of administration
nebulized Budesonide - ? any benefit
who should receive it? nedd clear cut indicators
26. Conclusion cause of much morbidity in pediatric population
potentially life-threatening
prompt diagnosis
assure adequate airway common and may be life-threatening
must make quick diagnosis on PE
airway first prioritycommon and may be life-threatening
must make quick diagnosis on PE
airway first priority