Download
1 / 41
420 likes | 495 Views
Measurement in STD research. Why Pool Specimens? . Pooling serum sample for HIV testing was found to be accurate and has been used to reduce the cost of enzyme linked immunoabsorbent assays (ELISA) for detection of antibody to HIV

E N D
Why Pool Specimens? • Pooling serum sample for HIV testing was found to be accurate and has been used to reduce the cost of enzyme linked immunoabsorbent assays (ELISA) for detection of antibody to HIV • To develop population estimates of disease prevalence and, in a multistep process, to determine which individual sample is positive
Tests Based on Genetic Markers • Non-amplified use a nucleic acid probe to detect the extremely small amount of an infectious organism’s unique genetic sequence (nucleic acid) • Amplified tests first make copies of the organism’s genetic sequence and magnify the “signal” of the organism (I.e. PCR, LCR • Less expensive and require less handling considerations than culture • May be less sensitive for some pathogens (but as good as culture for chlamydia and herpes) • FDA approved for CT, GC, and HIV
Surrogate Markers in AIDS Research • How do we study the relationship between immunologic and virologic parameters in HIV infected individuals? • Cross-sectional studies • Obscure or unknown relationship of the marker to HIV disease pathology • Technical barriers • Inherent complexity of the marker validation process
Surrogate Markers • CD4 cell counts • Weak as a surrogate marker: treatment- induced increases in CD4 cell counts only partially account for the improved clinical benefit seen with new therapies • HIV RNA Viral Load • Good indicator of antiretroviral drug activity • Strong predictor of clinical outcome
Discrepant Analysis • Discrepant analysis uses a combination of reference standards applied at two stages • Discordant cells are tested with the “gold standard” in an attempt to resolve the “discrepant” results
Discrepant Analysis • Advantages • Provides a cost savings (testing with the “gold standard” is not performed on all specimens • Limitations • Significant bias even under “ideal” conditions
Discrepant Analysis • Attempts to provide estimates of sensitivity and specificity in the presence of an imperfect gold-standard. • In the example of CT, apparent false positives are subjected to additional testing with DFA (direct immuno-fluorescence) or MOMP (major outer membrane protein) if any of these test positive than the original false is reclassified as true positive. • This analysis produces an upwardly biased estimate (Hadgu)
Discrepant Analysis Bias • Concordant specimens are not tested with the “gold standard” • These specimens are assumed to be true positives and true negatives – although they may not be • Not testing the concordant cells potentiall introduces bias – which direction?
Magnitude of the Bias • Amount of bias depends on the number of false results • False positive will occur more commonly with low prevalence • False negatives with high prevalence • Measured sensitivity and specificity will equal the true sensitivity and spcificity if: all false results of the new test must be discordant with results of the accepted standard (no misclassification of true positive or true negatives)
Effect of the Bias • Sensitivity is a concern with low disease prevalence • Specificity is a problem with high disease prevalence • (See Figure 1 in Miller, WC. Bias in discrepant analysis: when two wrongs don’t make a right. J Clin Epidemiol 1998;51:219-231)
Strategies to Reduce the Bias • If a “gold standard” exists – test all specimens using the GS • If no GS exists use the best “alloyed standard” or a combination of tests
Should we use Discrepant Analysis? • “Discrepant analysis should be avoided if at all possible” (Miller, WC) • What happens if a “gold standard” doesn’t exist? • Minimize bias through multiple testing using “alloyed standards”
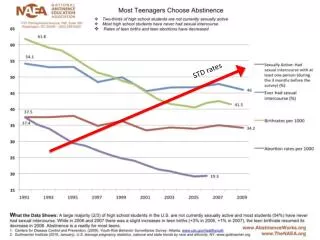
Contraception • Important in STD research because it causes behavior change • It is associated with lesser incentive to have protective sex • May have some protective effect in certain diseases. • 7 of 10 sexually active women do not want to become pregnant (AGI, 1988) • Unintended pregancies result in 1.4 abortions and 1.1 unwanted births. • 80% of teen pregnancies are unintended • Each year 1 in 10 15-19 year old girls become pregnant
Sterilization • Tubal • Vasectomy • Hysterectomy • No STI protection • Return to fertility is possible
Norplant - implants • levonorgestrel • last 5 years • prevents ovulation , causes luteal insufficiency, impaired oocyte maturation and progestin-induced hostile cervical mucus • No STI prevention • return to fertility is rapid
Depo provera • depot medroxyprogesterone acetate (DMPA) - The Shot • last 3-4 months • can cause menstrual changes, irregular bleeding, spotting, amenorrhea, headaches • return to fertility can be one year • No STI prevention
Emergency Contraception - Post Coital contraception • Has been available for 25 years. Could prevent 1.7 million unintended pregnancies and 800,00 abortions • OCPs taken (1st dose within 72 hours and 2nd dose 12 hours later) or IUD is inserted (up to 5 days after unprotected coitus) • Is not abortion. It delays ovulation
Abortion Pill • Only Mifepristone (RU486) is FDA approved • Antiprogesterone drug – a key hormone in the establishment and maintenance of pregnancy. Given with prostaglandins • Used up to 49-63 days from LMP • prevent implantation • No STI prevention
Oral Contraception • Prevents ovulation by suppressing pituitary gonadotropin secretion. • Monophasic - constant dose of estrogen and progestin in 21 active tablets • Progestin-only oral low dose contraceptives (mini-pills) • Phasic alter progestin and estrogen. • Associated with increased cervial chlamydia; protective against symptomatic PID
Health Benefits of OCP • Prevention of gynecologic cancer (epithelial ovarian cancer and endometrial adenocarcinoma) • Menstrual improvements (regularity, less dysmenorrhea, few days and amount of flow, less anemia, restoration of regular menses in anovulatory women) • Prevention of benign conditions (breast fibroadenoma, ectopic pregnancy) • Possible benefits (atherosclerosis, severe rheumatoid arthritis)
Intrauterine device • copper intrauterine implant Copper T 380A IUD - creates intrauterine environment that is spermicidal • progesterone-releasing IUD (Progestasert) inhibit sperm survival and implantation. • PID can result if CT or GC are present • No STI prevention
Natural Methods • Periodic abstinence (calendar method, temperature method, cervical mucus method, symptothermal method) • Lactational contraception • Withdrawal • None of these method provide STI prevention • Fertility return is rapid
Barrier Methods • Latex Condom • Diaphragms and cervical caps • spermicidal foams, films, jellies or suppositories • Do protect against STIs
Diaphragm and Cervical Cap • Diaphragm 80-94% effective • Cervical cap 60-90% effective • Not effective against STDs • can be messy • cost $13-$25, exam $150 • only four sizes of cervical caps (hard to fit all women)
Vaginal Contraceptive Film • Can't be felt by either partner • Effective for up to one hour • Nothing to remove Begins to dissolve instantly • Used by thousands of clinics • Contains: 28% Nonoxynol 9, the spermicide most recommended by doctors • Numerous clinical studies conducted worldwide on safety and efficacy
Male Methods • Condoms • Vasectomy • Others
Common invasive diagnostics • Gynecological exam • Colposcopy • Laparoscopy
Non-invasive diagnostics • Urine DNA amplification • Self-swabs • Self-administered tampons