Download
1 / 18
180 likes | 278 Views
Resection rate for patients with tissue confirmation of NSCLC (2004-2008:England). *adjusted for sex, age, PS, stage, deprivation index and Charlson co-morbidity index. Resection rate by PCT 2004-6*. *Source: National Cancer Data Repository. Mortality Hazard Ratios for Lung Cancer

E N D
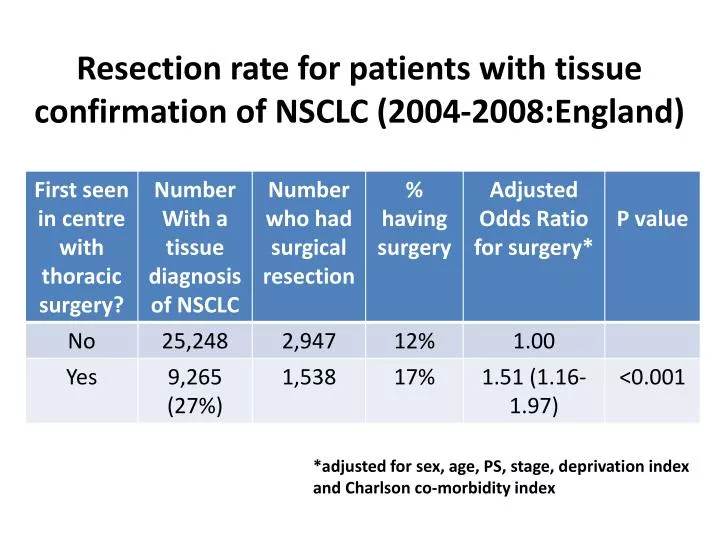
Resection rate for patients with tissue confirmation of NSCLC (2004-2008:England) *adjusted for sex, age, PS, stage, deprivation index and Charlson co-morbidity index
Resection rate by PCT 2004-6* *Source: National Cancer Data Repository
Mortality Hazard Ratios for Lung Cancer Patients in England 2004-6 related to resection rate by government office region N = 77,349
Mortality hazard ratios for resected patients; England 2004-6 by Government Regional Office N = 6,900
Mortality hazard ratios for resected patients; England 2004-6 by Government Regional Office Implications: comparing the top quintile PCT with Lower 4: 5420 deaths ‘postponed’ by surgery 146 deaths related to higher resection rates N = 6,900
The effects of investing in thoracic surgery on lung cancer resection rates Kelvin LauDavid WallerSridhar RathinamMichael PeakeGlenfield Hospital, Leicester, UK UK National Lung Cancer Audit Programme
There is a wide variation in lung cancer surgery in England 5.2% – 10.1% 10.9% – 13.2% 13.6% – 14.5% 14.6% – 16.5% 16.9% – 31.8%
Hypothesis the variability in Resection Rate is determined by the provision of specialist thoracic surgery Method We correlated results of the NATIONAL LUNG CANCER AUDIT with manpower data for cardiothoracic surgery
National Lung Cancer Audit results • 33 English Cancer Networks, comprising 174 Hospital Trusts • 31 Trusts had Thoracic Surgery in house (Base Hospitals) • 18 (58%) Trusts had less than 2 Pure Thoracic Surgeons • 13 (42%) Trusts had 2 or more Pure Thoracic Surgeons • In 2008, 15,774 cases of histologically confirmed NSCLC • 18.4% cStage I and II • 14.2% underwent resection
Resection rates are higher in centres who treat more cases R = 0.155 p = 0.06
Resection rates are higher in base than in referring centres Across the UK Within each Cancer Network p < 0.001 p < 0.001 Resection Rate
Resection rates are higher in centres with 2 or more specialist thoracic surgeons p = 0.02 Resection Rate
Resection rates are higher when surgeons attend preoperative MDTs p = 0.012
The increase in resection rate was greatest in those units who employed new thoracic surgeons p = 0.04 19% 66% 2009 Growth Resection Rate 2008
Conclusion • Lung cancer resection rates in UK can be increased by • Increasing the number of specialist thoracic surgeons at preoperative MDTs in referring hospitals • Increasing the number of specialist thoracic surgeons in operating centres • Thereby increasing the individual caseload in any unit • Individual Units must invest in more pure Thoracic Surgical appointments • The number of specialist thoracic surgeons in training must be increased
Resection Rate- Leicester * A Martin-Ucar et al. Lung Cancer. 2004; 46:227-232 (specialist thoracic surgeon appointed 1997)