Download
1 / 62
1k likes | 2.01k Views
CAROTID ARTERY DISEASE. Jehanzeb Bilal , MD PGY-3 Elias A. Iliadis , MD Medical Director, Noninvasive Vascular Intervention Cooper Heart Institute. Patient one. 49 year old female presents to her primary care physician for a routine check up. PMH: unremarkable.

E N D
CAROTID ARTERY DISEASE JehanzebBilal, MD PGY-3 Elias A. Iliadis, MD Medical Director, Noninvasive Vascular Intervention Cooper Heart Institute
Patient one • 49 year old female presents to her primary care physician for a routine check up. • PMH: unremarkable. • Social hx: smoker (1PP-30yrs). • Family History : CAD, HTN, CVA
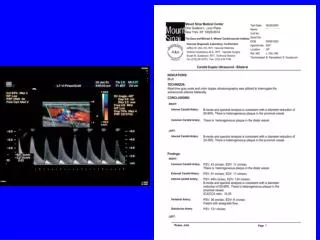
VS.:97 125/75 65 12 • Neurological exam : normal. • Cardiovascular : right carotid bruit. • The rest of the exam was unremarkable A carotid ultrasound was done.
The ultrasound revealed a 95 % stenosis of the left carotid.
Would you screen for carotid disease in asymptomatic patients? • What is the value of a carotid bruit on physical exam in an asymptomatic patient? • What is a hemodynamically significant carotid stenosis? • Would you further evaluate this patient ? • How would you manage her carotid stenosis?
The Framingham cohort • Evaluation of carotid bruit in this cohort • In eight years, a bruit appeared in 66 men and 105 women, all asymptomatic. • The incidence increased with age equally in the two sexes from 3.5% at 44 to 54 years, to 7.0% at 65 to 79 years. • The eight-year incidence was greater in diabetes and hypertensive subjects. • These patients had a stroke rate more than twice expected for age and sex. JAMA 1981 Apr 10;245(14):1442-5.
More often cerebral infarction occurred in a vascular territory different from that of the carotid bruit • Ruptured aneurysm, embolism from the heart, and lacunar infarction was the mechanism of stroke in nearly half the cases. • Incidence of myocardial infarction increased twofold . • General mortality increased; 1.7-fold with men, and 1.9-fold in women, with 79% of the deaths owing to cardiovascular disease, including stroke.
Conclusion of the study • Carotid bruit is clearly an indicator of increased stroke risk • General and non-focal sign of advanced atherosclerotic disease • Not necessarily an indicator of local arterial stenosis preceding cerebral infarction
The natural history of asymptomatic carotid artery occlusive lesions. • Follow up of 640 neurologically asymptomatic patients • 292 had pressure-significant internal carotid artery stenosis • 348 had a carotid bruit only without a pressure-significant lesion. • Patients with asymptomatic pressure-significant carotid stenosis are at greater risk for stroke than a non significant occlusion (twofold) and a general population (sevenfold). JAMA 1987Nov20;258(19):2704-7
The natural h/o carotid bruits in the elderly • To determine the relative risk for cerebrovascular events in elderly patients with carotid bruits • 241 NH residents were examined for carotid bruits and signs of previous stroke. • Twelve percent of residents had asymptomatic carotid bruits. • The 3-year cumulative incidence of strokes was 10%, vs. 9%, yielding a relative risk of 1.1 (95% CI, 0.45 to 2.7). • In 60% of surviving residents, baseline carotid bruits were no longer present at the time of follow-up examination. • The disappearance of these bruits was not associated with the occurrence of interval cerebrovascular events Ann Intern Med1990Mar12(5):340-3
SHEP • The Systolic Hypertension in the Elderly Program • To determine the association between asymptomatic carotid bruits and the development of subsequent stroke in older adults with isolated systolic hypertension. • 5-year randomized trial • Average follow-up 4.2 years. • Carotid bruits were found in (6.4%) of the participants . • Stroke developed in (7.4%) of those with carotid bruits and in (5.0%) of those without carotid bruits. J Gen Intern Med 1998 Feb;13(2):86-90
Relative risk of stroke with asymptomatic carotid bruits was 1.29 (95% CI 0.80, 2.06). • Subjects aged 60 to 69 years, trend (p=.08) toward increased risk (relative risk [RR] 2.05; 95% CI 0.92, 4.68) of subsequent stroke in persons with carotid bruits. • Subjects aged 70 or over, no relation between carotid bruit and subsequent stroke (RR 0.98; 95% CI 0.55, 1.76).
The causes and risk of stroke in patient with internal carotid artery stenosis • patients with unilateral symptomatic carotid-arterystenosis • Patients with asymptomatic contralateral stenosis • The risk of stroke at five years after study entry ina total of 1820 patients increased with the severity of stenosis. N Engl J Med 2000; 343:1420-1421, Nov 9, 2000.
Forty-five percentof strokes in patients with asymptomatic stenosis of 60 to 99percent are attributable to lacunes or cardioembolism.
Conventional angiography • Gold standard • Visualize the entire cerebrovascular system • Invasive test • Expensive test • Neurological morbidity/mortality
Non invasive carotid artery testing. A meta-analytic review. • Carotid angiography as the reference standard for comparison. • Carotid duplex ultrasonography, carotid Doppler ultrasonography, and magnetic resonance angiography are all similarly successful at predicting -100% carotid artery occlusion (SN 82 to 86,SP 98) -70% stenosis (SN 83 to 86,SP 89 TO 94 ) • Other factors, such as cost, availability, and local experience may influence the decision to use these tests to screen for carotid artery atherosclerosis that may respond to surgery Ann Intern Med 1995 Mar 1;122(5):360-7.
Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review • 64 studies reviewed. • MRA has a better discriminatory power compared with DUS in diagnosing 70% to 99% stenosis(SN95vs86/SP90vs87) • A sensitive and specific test compared with DSA in the evaluation of carotid artery stenosis. • For detecting occlusion, both DUS and MRA are very accurate.(SN 98 vs. 96/SP 100VS 100) Stroke 2003 May;34(5):1324-32.
Non-invasive imaging compared with intra-arterial angiography in the diagnosis of symptomatic carotid stenosis: a meta-analysis • CEMRA is superior to US,MRA and CTA, with SN 94 versus 89, 88, and 76 percent, respectively; specificities 93 versus 84, 84, and 94 percent, respectively Lancet. 2006 May 6;367(9521):1503-12
Carotid US • Least expensive • Easy to perform • Defines the plaque -The sensitivity and specificity are lower in asymptomatic patients -It can overestimate the stenosis: unnecessary surgery -Less precise in less than 50% stenosis, and total occlusion -It only defines cervical disease
MRA • May be more Sensitive and Specific than US (esp. CEMRA) • Disadvantage: -Cannot be done if patient is critically ill , or has a pacemaker -Expensive
CTA • Used when US is not reliable: -Severe calcific artery -Severe kinking of the vessels -Short neck -High bifurcation -Overview of surgical field
Can we bypass invasive angiography? • Separate and combined test results of DUS and MRA were compared with the reference standard DSA. Only the stenosis measurements of the arteries on the symptomatic side were included in the analyses. • When MRA and DUS were combined , agreement between these 2 modalities (84% of patients) gave a sensitivity of 96.3% (95% CI, 90.8% to 99.0%) and a specificity of 80.2% (95% CI, 73.1% to 87.3%) for identifying severe stenosis(>70) • This combination may obviate the need of an invasive angiography ,if the results of both tests were similar. Stroke 2002 Aug;33(8):2003-8.
Guidelines • The United States Preventive Services Task Force (USPSTF) recommends against screening for asymptomatic carotid artery stenosis in the general population . • The American Heart Association and American Stroke Association acknowledge that "screening of general populations for asymptomatic carotid stenosis is unlikely to be cost-effective" . • The American Society of Neuroimaging suggests that, while screening for the general population is not recommended, screening might be considered for patients ≥65 years with significant risk factors for cardiovascular disease .
PREVENTION OF STROKES IN ASYMPTOMATIC BUT HEMODYNAMICALLY SIGNIFICANT CAROTID ARTERY STENOSIS.
VA STUDY • Multicenter clinical trial • 444 men with asymptomatic carotid stenosis shown arteriographically (50 percent or more). • Randomly assigned to optimal medical treatment including ASPIRIN plus carotid endarterectomy ( 211 patients) or optimal medical treatment alone (233 patients) • The incidence of ipsilateral neurologic events was 8.0 percent in the surgical group and 20.6 percent in the medical group (P 0.001), RR of 0.38 (95 confidence interval,( 0.22 to 0.67). N Engl J Med 1993 Jan 28;328(4):221-7
ACAS(asymptomatic carotid atherosclerosis study) • Randomized, multicenter trial • Total of 1662 patients with asymptomatic carotid artery stenosis of 60% or greater • medical risk factor management for all patients; carotid endarterectomy for patients randomized to receive surgery. • After a median follow-up of 2.7 years, the incidence of ipsilateral stroke and any perioperative stroke or death rate was significantly lower in the surgical group than with aspirin alone (5 versus 11 percent) for a relative risk reduction of 0.53 (95% CI 0.22-0.72). • Men had an absolute risk reduction of 8 percent; the absolute risk reduction in women was only 1.4 percent. JAMA 1995 May 10;273(18):1421-8
ACST (asymptomatic carotid surgery trial) • 3120 asymptomatic patients with 60% stenosis(US) • randomized between immediate CEA and indefinite deferral of any CEA (4% per year)and were followed for up to 5 years. • The net five-year risk for all strokes or perioperative death in the CEA group was reduced by nearly half. • The absolute risk reduction over five years was greater for men than for women 8.2 percent versus 4.08 Lancet 2004 May 8;363(9420):1491-502.
COCHRANE REVIEW • All completed randomized trials comparing CEA to medical treatment in patients with asymptomatic carotid stenosis • 5223 patients were included. • Despite about a 3% perioperative stroke or death rate, CEA for asymptomatic carotid stenosis reduces the risk of ipsilateral stroke, and any stroke, by approximately 30% over three years. • The absolute risk reduction is small (approximately 1% per year over the first few years of follow up in the two largest and most recent trials) but it could be higher with longer follow up. Cochrane Database Syst Rev 2005;(4):CD001923
Factors to consider in assessing risk and benefit of CEA • Exclusion criteria (life expectancy of < five years) • The severity of stenosis. • The presence of newer drugs. • The frequency of TIA in carotid disease.
The differentiation between the nature of stroke(cardioembolic and lacunar). • The controlateral carotid artery. • The Late benefit of CEA. • The gender. • Postoperative complications.
Guidelines • For asymptomatic patient with a stenosis of 60 to 99 %,CEA is recommended only for patients aged between 45 and 75 with a life expectance of at least five years. NNT 33 • The benefit of CEA appears only after couple of year. • ASA should be used pre and postoperatively.
Patient two • 69 y old female was found to have b/l carotid bruit on physical exam. She has no history of strokes or transient ischemic attack. • PMH: CAD with triple vessel disease , CHF with diastolic dysfunction, DM, HTN, dyslipidemia. • She is a past smoker(40 p/year) • Meds: coreg, simvastatin, lisinopril, insulin, asa, lasix.
A carotid ultrasound and a conventional angiography showed a severe stenosis(more than 95%) of her right ICA , • Is she a candidate for a CEA? What is the current data on Carotid Artery Stenting?
SAPHIRE(stenting and angioplasty with protection in patients at high risk of endarterectomy • A randomized trial comparing carotid-artery stenting with the use of an emboli-protection device to endarterectomy • 334 patients with coexisting conditions that potentially increased the risk posed by endarterectomy and who had either a symptomatic carotid-artery stenosis of at least 50 percent of the luminal diameter or an asymptomatic stenosis of at least 80 percent. • More than seventy percent of patients had asymptomatic disease. • Twenty percent had a restenosis after CEA. N Engl J Med 2004 Oct 7;351(15):1493-501.
The primary end point was a combined incidence of death, stroke and MI in the first thirty days postoperatively or death/ipsilateral stroke from day 31 up to one year. • The study was designed to test the non-inferiority of CAS to CEA in this population.
The primary end point occurred in 20 patients randomly assigned to undergo carotid artery stenting and in 32 patients randomly assigned to undergo endarterectomy (P=0.004 for noninferiority, and P=0.053 for superiority). • At one year, carotid revascularization was repeated in fewer patients who had received stents than in those who had undergone endarterectomy (P=0.04). • CAS is non inferior to CEA in patient with carotid artery disease and high risk for surgery.
The FDA approved the stent used in this trial for high risk patients with carotid disease.
Guidelines • CAS should be considered in patients with severe carotid stenosis(>70%) and one of the following conditions: -Severe medical comorbidities(cardiopulmonary). -Difficult neck access for CEA. -Stenosis after irradiation. -Restenosis after CEA. -Contralateral laryngeal palsy.
Patient three • 57 year old male presents to the ER with acute weakness of his right arm and leg .The symptoms started 12 hour ago. • He has a h/o of HTN and dyslipidemia, currently on lisinopril and simvastatin. • Physical exam:97 170/100 85 15 -He had a 4/5 weakness of his right arm and leg -Cardiovascular exam was unremarkable
CT scan of the brain without contrast showed chronic small vessel disease. • MRI brain revealed an acute infarct of left middle cerebral artery territory. • MRA showed an 90 % stenosis of his left carotid artery. • He was admitted to the stroke unit.
Is the management of carotid disease different in symptomatic patients?
NASCET TRIAL(North American Symptomatic Carotid Endarterectomy Trial) • 659 patients with a h/o of stroke in the past 120 days • had 70-90 %stenosis of the ipsilateral carotid artery. • Patients were randomized to medical management vs. medical management with CEA. • The primary outcome was any stroke or death. • The study was prematurely terminated by the NIH because of the clear evidence of benefit from surgery . • At the time of study termination, patients had been followed for a mean of 18 months. N Engl J Med 1991 Aug 15;325(7):445-53
The risk of stroke and death was higher at 30 days in the patients treated with CEA (5.8 versus 3.3 percent with medical therapy) • longer follow-up revealed a lower cumulative risk at two years of any ipsilateral stroke (9 versus 26 percent, p<0.001) • A lower risk of major or fatal ipsilateral stroke (2.5 versus 13.1 percent, p<0.001)