Download
1 / 40
400 likes | 555 Views
Priorities in TB Research Dermot Maher, Senior Clinical Epidemiologist, Medical Research Council / Uganda Virus Research Institute, Entebbe, Uganda. 13 th Turkish Thoracic Society Congress Istanbul, 8 May 2010. Mycobacterium tuberculosis ( Credit: Clifton E. Barry III).

E N D
Priorities in TB Research Dermot Maher, Senior Clinical Epidemiologist, Medical Research Council / Uganda Virus Research Institute, Entebbe, Uganda 13th Turkish Thoracic Society Congress Istanbul, 8 May 2010
Introduction - importance of TB research Need for more and better TB research Scope of TB research Research and development XDR-TB research agenda TB/HIV research agenda Conclusion – Research Movement to Stop TB Contents
1415 species of infectious organisms known to be pathogenic to humans: 217 viruses and prions 538 bacteria and rickettsia 307 fungi 66 protozoa 287 helminths (Taylor et al. Phil Trans R Soc Lond 2001; 356: 983-989) One among many…...
but a “captain of the men of death” Globally in 2008 an estimated: • 9.4 million new cases (including 500,000 MDR-TB) • 1.8 million deaths (including 500,000 HIV-positive)
In 1986 Professor Wallace Fox retired and the MRC closed the Tuberculosis Unit (Professor Denny Mitchison’s laboratory unit had been effectively closed 12 months previously). Problem solved? It might have seemed reasonable to think so at the time, but no-one knew what lay ahead. 1986 – the end of an era of progress, the beginning of an era of indifference Wallace Fox 1920-2010
Need for more and better TB research Current technology for TB control is old: • 1882 sputum smear microscopy (Koch) • 1895 X-rays (Röntgen) • 1922 BCG • 1970s rifampicin (last new widely used TB drug) Research is necessary to: • make the most of current approaches to TB control (epidemiological, programmatic and policy research); • develop the new "tools" for TB control (diagnostics, drugs and vaccines); • revolutionize TB control technology to achieve the goal of TB elimination by 2050. Current scope, scale and speed of TB research is inadequate due to inadequate funding and insufficient commitment by many institutions.
Global expenditures on health R&D(Science 2006, 311, 162-167)
$158 million TB $183 million anthrax $187 million smallpox $2.9 billion HIV NIH research funding , 2005
NIH 2005 Research expenditures (US$ billions)(Treatment Action Group, 2006)
Scope of TB research Basic research Development of new tools (drugs, vaccines, diagnostic tests) Implementation research (health policy, systems and service delivery) Monitoring and evaluation of impact WHO/CDS 2000
Basic research Laboratory research aimed at increasing understanding of the biology of M. tuberculosis and its interaction with the human host. e.g. How does drug resistance affect virulence and reproductive fitness? Basic research generates the drug candidates entering the R&D pipeline: hit -> lead -> drug candidate How can genomics inform target-based screening in the drug discovery strategy?
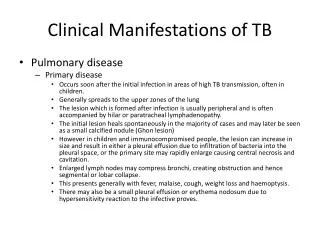
“Understanding how M. tuberculosis lies quiescent for years if not decades, how the immune system fails to detect and eradicate it, and the nature of the stimuli for its reactivation remain nearly as uncertain today as in Robert Koch’s time”. Bishai WR. Rekindling old controversy on eluisve lair of latent tuberculosis. (Commentary). Lancet 2000; 356: 2113-2114. Understanding latency
Development of new tools (drugs, vaccines, diagnostic tests)
Anti-TB drugs introduced following streptomycin • p-aminosalicylic acid (1949) • isoniazid (1952) • pyrazinamide (1954) • cycloserine (1955) • ethambutol (1962) • and rifampicin (1963) then NOTHING for 40 years
New drugs First the good news Development pipeline for anti-TB drugs is better supplied than ever before, with 10 compounds in clinical development (Spigalman M. New tuberculosis therapeutics: a growing pipeline. J Infect Dis 2007; 196 (suppl 1): 28-34)
New drugs and then the bad.... Probably too few to guarantee even a single new anti-TB drug by 2010 (Glickman SW et al. A portfolio model of drug development for tuberculosis. Science 2006; 311: 1246-7)
Vaccines BCG • decreases risk of progression of M. tuberculosis infection to disease • protects children against severe/disseminated TB • is unlikely to protect for more than 15 years • often has low efficacy against PTB in adults
New TB vaccines: potential modes of action prevent infection prevent primary disease prevent latency prevent reactivation WHO/CDS 2000
New TB vaccines under development: recombinant BCG vaccinesnew recombinant fusion proteins given with new adjuvantsnon-replicating or replication-deficient viral-vectored vaccinesweakened Mycobacterium tuberculosis (instead of the weakened Mycobacterium bovis used in BCG) WHO/CDS 2000
Diagnosis of infection T cell-based interferon gamma release assays (IGRA) Production of interferon gamma by T cells in response to two antigens, ESAT-6 and CFP-10 • ELIspot, e.g. T-SPOT.TB • ELISA, e.g. QuantiFERON-TB Gold
Diagnosis of drug-resistant TB Standard culture & drug sensitivity testing (DST) 2-3 months from sputum collection to results Delayed recognition of drug resistance Limited reproducibility and accuracy of DST for 2nd line anti-TB drugs Risk of ineffective treatment Risk of transmission of drug-resistant strains to others
New tests for diagnosis of drug-resistant TB: microscopic-observation drug susceptibility (MODS) Liquid culture assay Microscopic observation of a cording pattern unique to M. tuberculosis (aggregation of TB bacilli forming serpentine structures) Median time for disease identification and DST = 7 days Cost < $2 per test Moore D, Evans CA, Gilman RH, et al. Microscopic-observation drug susceptibility assay for the diagnosis of TB. N Eng J Med 2006; 355: 1539-50.
New tests for diagnosis of drug-resistant TB: molecular methods Focus on identification of rifampicin resistance as a surrogate marker for potential resistance to other drugs: Line-probe hybridisation assay, e.g. Hain Genotype MTBDRplus Molecular beacon assay Luciferasemycobacteriophage strategy Dideoxy fingerprinting Direct sequencing of PCR products Jassal M, Bishai WR. Extensively drug-resistant tuberculosis. Lancet Infect Dis 2009; 9: 19-30.
MTB New diagnostic tools for DRTB Direct NRA (“Griess”) MODS MGIT MTBDR-PLUS (“Hain”) Xpert MTB/RIF (Cepheid)
Operational research “Increasingly, infectious disease research will be linked to the development of the medical infrastructure and training needed in developing countries to translate scientific advances into operational reality.” Anthony Fauci Director, National Institute of Allergy and Infectious Diseases, Bethesda, USA Fauci A. Clinical Infectious Diseases 2001; 32: 675-85 WHO/CDS 2000
Operational research Research to improve TB control activities Solutions to context-specific problems Collaboration between TB programme and researchers International Union Against TB & Lung Disease Centre for Operational Research www.theunion.org/research-and-policy/centre-for-operational-research.html WHO/CDS 2000
NIAID research agenda on MDR/XDR-TB, 2007 • develop and test reliable technologies to rapidly diagnose TB and identify drug resistance • define most effective use of current 2nd line TB treatments and develop new anti-TB drugs • understand the basic biology and immunology of host and pathogen that underlie development and spread of drug-resistant strains • understand epidemiology and programmatic determinants of drug resistance • determine the influence of HIV on development of drug resistance and on treatment outcomes • develop effective chemoprevention and vaccines
“We are calling on the world to recognize that we can’t fight AIDS unless we do much more to fight TB”July 14, 2004Durban, South Africa
TB/HIV research agenda • Improve diagnosis of TB among people with HIV • Maximise TB case-finding • Optimise TB preventive therapy • Determine optimal timing of ART after starting TB treatment • Improve detection and management of IRIS • Ensure performance of new diagnostics, drugs and vaccines in people with HIV • Improve HIV & TB programme collaboration • Improve HIV & TB surveillance
TB research priorities: in summary (1) Progress in TB research…. in the late 19th and early 20th century with state funding for diagnostics and vaccine development in the mid-20th century with state funding for drug development Stagnation in TB research…. since the 1970s and the development of rifampicin
TB research priorities: in summary (2) Until signs of renaissance in TB research… in the early years of the 21st century with public-private partnerships for new tools to speed up progress towards targets for 2015 But… much more funding is needed overall and specifically for basic research and operational research So… we need to harmonise research efforts and boost research funding through the Research Movement to STOP TB
Research Movement to Stop TB http://www.stoptb.org/researchmovement/