Download
1 / 2
20 likes | 123 Views
Case of the week 08-16:Advanced late gadolinium enhancement optimisation. History: 48 Y/O male from Kuwait presented with dyspnea and palpitations. Holter shows 2:1 heart block episodes. PMH: severe asthma. Echo : LV impairment with regional wall motion abnormalities

E N D
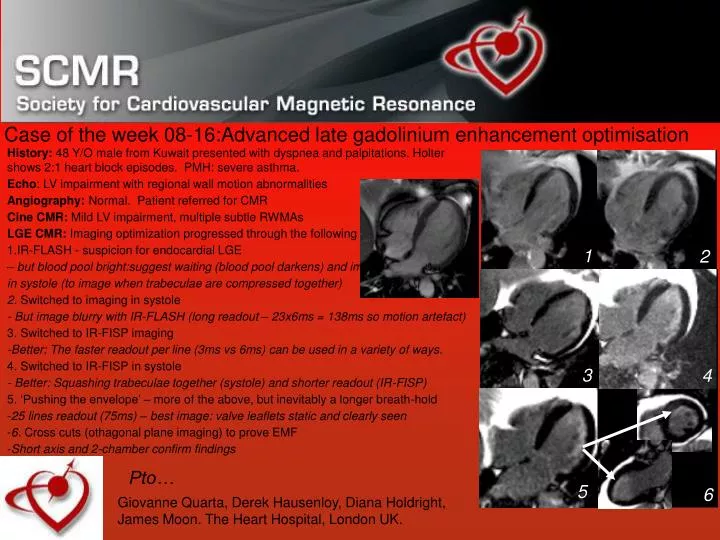
Case of the week 08-16:Advanced late gadolinium enhancement optimisation • History: 48 Y/O male from Kuwait presented with dyspnea and palpitations. Holter shows 2:1 heart block episodes. PMH: severe asthma. • Echo: LV impairment with regional wall motion abnormalities • Angiography: Normal. Patient referred for CMR • Cine CMR: Mild LV impairment, multiple subtle RWMAs • LGE CMR: Imaging optimization progressed through the following steps: • IR-FLASH - suspicion for endocardial LGE • – but blood pool bright:suggest waiting (blood pool darkens) and imaging • in systole (to image when trabeculae are compressed together) • 2. Switched to imaging in systole • - But image blurry with IR-FLASH (long readout – 23x6ms = 138ms so motion artefact) • 3. Switched to IR-FISP imaging • -Better: The faster readout per line (3ms vs 6ms) can be used in a variety of ways. • 4. Switched to IR-FISP in systole • - Better: Squashing trabeculae together (systole) and shorter readout (IR-FISP) • 5. ‘Pushing the envelope’ – more of the above, but inevitably a longer breath-hold • 25 lines readout (75ms) – best image: valve leaflets static and clearly seen • 6. Cross cuts (othagonal plane imaging) to prove EMF • Short axis and 2-chamber confirm findings 1 2 3 4 Pto… 5 6 Giovanne Quarta, Derek Hausenloy, Diana Holdright, James Moon. The Heart Hospital, London UK.
Case of the week 08-16:Tips and tricks: LGE in endomyocardial fibrosis: 2 of 2 CMR diagnosis: Probable endomyocardial fibrosis: consider filiarial disease, Churgg-Strauss. What was the eosinophil count? Follow-up: Eosinophils normal: Unfortunately patient returned to home country before full investigation. CMR perspective. Advanced practionners of CMR can get the most out of LGE imaging by taking many images and adjusting the acquisitions for both for patient characteristics and the disease under investigation. An SSFP readout is twice as fast and frequently this permits increased optimisation. See table below for our basic imaging modifications for specific clinical situations (using a Siemens Avanto scanner).