Download
1 / 1
30 likes | 226 Views
Contrast Induced Nephropathy (CIN), is it a concern for patients undergoing CT- pulmonary angiography (CT/PA )?. Upul Madampage ¹ and J. Kappel ¹ , ² 1 Department of Internal Medicine, Royal University Hospital, University of Saskatchewan, Saskatoon, SK, Canada.

E N D
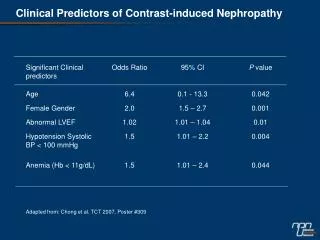
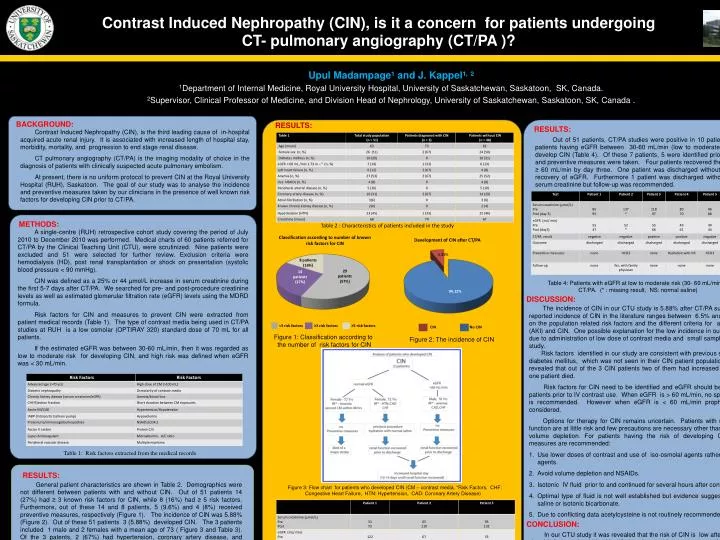
Contrast Induced Nephropathy (CIN), is it a concern for patients undergoing CT- pulmonary angiography (CT/PA )? UpulMadampage¹ and J. Kappel¹, ² 1Department of Internal Medicine, Royal University Hospital, University of Saskatchewan, Saskatoon, SK, Canada. 2Supervisor, Clinical Professor of Medicine, and Division Head of Nephrology, University of Saskatchewan, Saskatoon, SK, Canada . BACKGROUND: RESULTS: RESULTS: Contrast Induced Nephropathy (CIN), is the third leading cause of in-hospital acquired acute renal injury. It is associated with increased length of hospital stay, morbidity, mortality, and progression to end stage renal disease. CT pulmonary angiography (CT/PA) is the imaging modality of choice in the diagnosis of patients with clinically suspected acute pulmonary embolism. At present, there is no uniform protocol to prevent CIN at the Royal University Hospital (RUH), Saskatoon. The goal of our study was to analyse the incidence and preventive measures taken by our clinicians in the presence of well known risk factors for developing CIN prior to CT/PA. Out of 51 patients, CT/PA studies were positive in 10 patients. There were 7 patients having eGFR between 30-60mL/min (low to moderate risk) who did not develop CIN (Table 4). Of these 7 patients, 5 were identified prior to the procedure and preventive measures were taken. Four patients recovered their eGFR levels to ≥ 60 mL/min by day three. One patient was discharged without follow-up prior to recovery of eGFR. Furthermore 1 patient was discharged without post-procedure serum creatinine but follow-up was recommended. METHODS: Table 2 : Characteristics of patients included in the study A single-centre (RUH) retrospective cohort study covering the period of July 2010 to December 2010 was performed. Medical charts of 60 patients referred for CT/PA by the Clinical Teaching Unit (CTU), were scrutinized. Nine patients were excluded and 51 were selected for further review. Exclusion criteria were hemodialysis (HD), post renal transplantation or shock on presentation (systolic blood pressure < 90 mmHg). CIN was defined as a 25% or 44 µmol/L increase in serum creatinine during the first 5-7 days after CT/PA. We searched for pre- and post-procedure creatinine levels as well as estimated glomerular filtration rate (eGFR) levels using the MDRD formula. Risk factors for CIN and measures to prevent CIN were extracted from patient medical records (Table 1). The type of contrast media being used in CT/PA studies at RUH is a low osmolar (OPTIRAY 320) standard dose of 70 mL for all patients. If the estimated eGFR was between 30-60mL/min, then it was regarded as low to moderate risk for developing CIN, and high risk was defined when eGFR was < 30 mL/min. Classification according to number of known risk factors for CIN Development of CIN after CT/PA Table 4: Patients with eGFR at low to moderate risk (30- 60 mL/min ) prior to CT/PA. (* : missing result, NS: normal saline) DISCUSSION: The incidence of CIN in our CTU study is 5.88% after CT/PA suspected PE. The reported incidence of CIN in the literature ranges between 6.5% and 19% depending on the population related risk factors and the different criteria for acute kidney injury (AKI) and CIN. One possible explanation for the low incidence in our hospital, may be due to administration of low dose of contrast media and small sample size of our CTU study. Risk factors identified in our study are consistent with previous studies except for diabetes mellitus, which was not seen in their CIN patient population. We have also revealed that out of the 3 CIN patients two of them had increased hospital stay and one patient died. Risk factors for CIN need to be identified and eGFR should be calculated on all patients prior to IV contrast use. When eGFR is > 60 mL/min, no specific prophylaxis is recommended. However when eGFR is < 60 mL/min prophylaxis should be considered. Options for therapy for CIN remains uncertain. Patients with near normal renal function are at little risk and few precautions are necessary other than the avoidance of volume depletion. For patients having the risk of developing CIN the following measures are recommended: Use lower doses of contrast and use of iso-osmolal agents rather than low osmolal agents. Avoid volume depletion and NSAIDs. Isotonic IV fluid prior to and continued for several hours after contrast. Optimal type of fluid is not well established but evidence suggests use of isotonic saline or isotonic bicarbonate. Due to conflicting data acetylcysteine is not routinely recommended. <3 risk factors ≥3 risk factors ≥5 risk factors CIN No CIN Figure 1: Classification according to the number of risk factors for CIN Figure 2: The incidence of CIN Table 1: Risk factors extracted from the medical records RESULTS: General patient characteristics are shown in Table 2. Demographics were not different between patients with and without CIN. Out of 51 patients 14 (27%) had ≥ 3 known risk factors for CIN, while 8 (16%) had ≥ 5 risk factors. Furthermore, out of these 14 and 8 patients, 5 (9.6%) and 4 (8%) received preventive measures, respectively (Figure 1). The incidence of CIN was 5.88% (Figure 2). Out of these 51 patients 3 (5.88%) developed CIN. The 3 patients included 1 male and 2 females with a mean age of 73 ( Figure 3 and Table 3). Of the 3 patents, 2 (67%) had hypertension, coronary artery disease, and congestive heart failure. Only 1 of them had anaemia. Out of 3 patents, 2 patients had eGFR (> 60 mL/min) prior to procedure and only 1 of them was treated with pre- and post-procedure hydration using normal saline. One out of these two CIN patients died after four days due to major hemorrhagic stroke. Figure 3: Flow chart for patients who developed CIN (CM – contrast media, *Risk Factors, CHF: Congestive Heart Failure, HTN: Hypertension, CAD: Coronary Artery Disease) CONCLUSION: In our CTU study it was revealed that the risk of CIN is low after CT/PA. However the risk factors should be identified and preventive measures undertaken if eGFRis <60 mL/min. If eGFR is > 60 mL/min and risk factors ≥3 preventive measures should be undertaken. The development of a protocol may be helpful in the care of these patients. ACKNOWLEDGEMENTS: Merne Wilson (RN, BScN, MSc) Table 3 : Characteristics of CIN patients



![ARMYDA-CIN Trial [ Atorvastatin for Reduction of Myocardial Damage during Angioplasty–Contrast-Induced Nephropathy ]](https://cdn0.slideserve.com/625136/slide1-dt.jpg)