Download
1 / 27
300 likes | 651 Views
Patient Restraints and Restrictive practices Policy No. 503.073. Philosophy – cont.

E N D
Patient Restraints and Restrictive practicesPolicy No. 503.073
Philosophy – cont. The organization seeks to prevent, reduce, and eliminate the use of restraints or restrictive practices. Restraints should be used only to protect the patient’s health and safety while preserving the dignity, rights and well-being of the patient.
Alternatives to restraints • Offer/assist to bathroom or commode • Diversional activities • Consider sources of confusion – medications, pain, infection, hypoxia
Alternatives to restraints • Cover tubes • Relaxation techniques • Contact physician for further intervention • Personal alarms/bed alarms
Alternatives to restraints • Reorientation • Frequent contact • Move closer to nurses station • Family/sitter
Alternatives to restraints • Visual reminders • Reposition or ambulate • Decrease stimulation • Obtain a physician’s order to remove any unnecessary tubes
Four typesof restraints • Physical • Chemical • Seclusion • Therapeutic Holding/Physical redirection
Assessment/Reassessment criteria All patients will have an assessment performed to determine safety and protective needs prior to the application of restraints, including patient and family as appropriate. The use of restraints will be frequently evaluated and discontinued at the earliest possible time based on the assessment of the patient’s condition.
Physical Any manual method or physical or mechanical device, material or equipment that immobilizes or reduces the ability of a patient to freely move his or her arms, legs, body or head freely.
The following are not considered restraints • Orthopedic devices • Protective helmets • Methods that involve the physical holding of a patient for the purpose of conducting routine physical exams or tests.
The following are not considered restraints • Using all four side rails for patients in specialty beds, i.e. stretchers or patients experiencing involuntary movements, i.e. padded siderails for seizure activity.
The following are not considered restraints • Forensic and corrective restrictions imposed by correction authorities. • Age appropriate child care equipment such as: crib rails or swing, stroller and high chair safety belts.
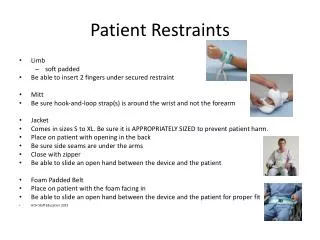
Application of restraining devices • Secure the limb restraint to the part of the bed frame that moves up when the head of the bed is elevated. • Secure the limb restraint with a quick release knot like the slip knot. • Do not tie in a knot!
Leather restraints • If using a locked restraint device verify you have immediate access to the key.
Indications for removal of restraints • When the patient demonstrates a change in the behavior that was the reason for the initial application. • If the behavior has decreased so the risk to the patient and others is no longer present the restraint may be removed.
Chemical Any medication that is used as a restriction to manage the patient’s behavior or restrict the patient’s freedom of movement and is not *standard treatment or dosage for the patient’s condition.
Seclusion The involuntary confinement of a patient alone in a room or an area where the person is physically prevented from leaving. • Used in the Emergency Department
Therapeutic holding/physical redirection The process of holding a patient in a manner that restricts movement
Leadership Notification and Reporting Requirements • The Department Director or Clinical Coordinator will be notified of potential need for use of restraints prior to application except in an emergency situation • The Department Director or Clinical Coordinator will evaluate whether additional resources are required to facilitate discontinuation of restraints or minimize recurrent episode.
Monitoring & Reassessment- timeframes • Maintenance of Therapy/Promotion of Healing- is monitored every two hours • Violent and Self-Destructive -require an initial assessment when restraints are initiated then every 15 minutes thereafter
Monitoring and reassessment- requirements • Signs of physical and psychological distress, i.e. positional asphyxia, will be recognized and responded to in accordance with the Rapid Response policy PCM - 503.200, CPI training and department specific Violence Control plans.
First Aid Interventions • For minor injuries such as; bruises, cuts or scrapes • Contact the physician for treatment orders. • Adhere to Skin impairment policy- PCM policy 502.007 • Pressure ulcer prevention - PCM-502.007
Monitoring and reassessment- requirements • General well-being • Respiratory/Circulatory status • Need for fluid/food hydration • Social needs or requests • Potential for release/ removal • Vital signs • Comfort • Signs of injury associated with restrictive practice
Transportation of restrained patients • Restraints will be maintained throughout transport with the appropriate intensity of observation • When restraints need to be removed for tests or procedures/treatments, the patient will be observed during that period & restraints reapplied prior to transport back to the unit • Documentation will continue as appropriate for the patient & type of restrictive practice • Upon returning to the department the restraint application will be reevaluated
Staff Education • All staff having direct patient contact must have: • Crisis Prevention Intervention training • First Aid training • CPR training