Download
1 / 52
580 likes | 1.52k Views
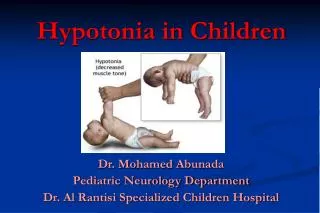
Children with Hypotonia. + Domains -. Dimensions. NDT Enablement Classification Model of Health and Disability. From: NDT Approach Theoretical Foundations & Principles of Clinical Practice, Table 2.1 pg. 82. Hypotonia. May:. Be transient and disappear Preterm infants

E N D
M R Franjoine & M P Haynes + Domains- Dimensions NDT Enablement Classification Model of Health and Disability From: NDT Approach Theoretical Foundations & Principles of Clinical Practice, Table 2.1 pg. 82
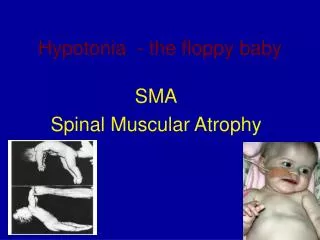
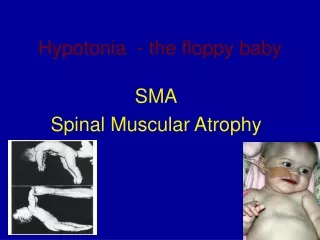
Hypotonia May: • Be transient and disappear • Preterm infants • Medically fragile children • Continue as Hypotonic CP • Later be diagnosed as Athetoid, Ataxic, or Spastic CP
Hypotonia May: • Be part of an obvious or later diagnosed genetic syndrome • Down Syndrome • Prader-Willi • Joubert Syndrome • Other syndromes • Fetal alcohol syndrome (FAS) • Fragile X syndrome • Maternal drug abuse
Hypotonia • A muscle fiber type disorder • Sensory integration disorder • MR • Autism May be:
Body Structure and Functions • Cognition • Neuromuscular System • Sensory System • Musculoskeletal System • Regulatory • Gastrointestinal • Cardiopulmonary • Integumentary
Cognition • Variable: • Child to child • Etiology • Cognition often underestimated • Flat affect • Appears “slow” or “lazy” • Latency of response time
What is Hypotonicity? • Abnormally low muscle resting tone • Abnormally low resistance to being lengthened • Feels “soft” when handled • Described as “floppy”
Neuromuscular System --Primary Impairments • Impaired Muscle Activation Insufficient Co-activation • Impaired Muscle Synergies • Inability to Initiate, Sustain, Terminate
Inadequate Co-activation • Holding joint positions in midrange is difficult • Move quickly through transitions • Tend to work at end ranges • Decrease degrees of freedom distally • Hyperextention of elbows and knees
Initiate, Sustain, Terminate • Difficulty initiating muscle contraction • Threshold for fiber firing • Insufficient number of fibers recruited • Slow to respond • Response is then short-lived • “Good baby”…later “lazy” • May have a flat affect • In supine “look flat”
Initiate, Sustain, Terminate • Difficulty in sustained holding against gravity…especially postural muscles • Look like gravity is pulling them down • Have a “belly” when upright • Often turns muscles off to quickly • i.e. Collapse when standing
Neuromuscular System • Impaired Motor Execution • Impaired Modulation and Scaling of Forces • Impaired Timing and Sequencing • Excessive overflow of Intra-Interlimb contractions
Impaired Modulation andScaling of Forces • Phasic bursts of movement • Little grading – moves quickly to end ranges • Overshoots target or strikes target inappropriately
Impaired Timing and Sequencing • Primary— • Difficulty grading agonists and antagonists • Timing and sequencing difficulties may be secondary to initiate, sustain, and strength issues
Neuromuscular System • Impaired Force Generation • Strength: the ability to contract a muscle to a sufficient degree to impact the task • Primary • inability to reach threshold for muscle firing • inability to recruit enough muscle fibers • Secondary • Little muscle holding: decreased strength/atrophy • Changes in muscle fiber type 2°to phasic use
Neuromuscular System • Anticipatory Postural Control— Probably not a primary impairment • Difficult with latency of initiation • Often they may anticipate a movement and “lock out their joints” in anticipation • Anticipation may be present…just not appropriate
Neuromuscular System • Poverty of Movement • “Poverty”--they don’t move much • Happy to stay in one place • Movement repertoires are somewhat limited • Secondary to strength, alignment, and stability available to them during development • Movements in the frontal and, especially, the transverse planes are less frequently seen
Neuromuscular System • Fractionated or Dissociated Movements • Often use pure reciprocal innervation rather than co-contraction • Movements may be “too dissociated” • Need to control degrees of freedom to support purposeful isolated control • Often fix distally • Splaying of fingers • Plantar-flexion of ankles
Sensory System Vision • Vestibular • Somatosensory
Vision • Primary Impairments • Refractory errors • Visual field loss • Strabismus • Cortical visual impairment not as common as in SQ • Secondary Impairment • Uses eyes for postural stabilization
Somatosensory • Difficulty using: • proprioceptive information • tactile information • Primary impairment • If inappropriate firing of receptors • Secondary impairment • If caused by lack of experience due to little movement, ability to read the input didn’t develop well
Sensory Processing • “ the ability of the nervous system to perceive, interpret, modulate, and organize sensory input for use in generating or adapting motor responses… (Miller & Lane 2000) • Degree of difficulty varies widely by etiology of the hypotonia
Musculoskeletal System • Bones: • Changes are usually secondary to static positons • Plagiocephaly • Flattend ribcage • Kyphosis • Shoulder instability • Hip instability
Musculoskeletal System • Muscles: • Atrophy • Weakness • Fiber type changes • Muscle shortening • Muscle overlengthening • Connective tissue:
Musculoskeletal System • Muscles: • Atrophy • Weakness • Fiber type changes • Muscle shortening • Muscle overlengthening Primary or Secondary Impairments?
Musculoskeletal System • Connective Tissue: • Hyperextensible joints • Ligamentous laxity Primary or Secondary Impairments?
M R Franjoine & M P Haynes + Domains- Dimensions NDT Enablement Classification Model of Health and Disability From: NDT Approach Theoretical Foundations & Principles of Clinical Practice, Table 2.1 pg. 82
General Characteristics of Posture in Children with Hypotonia • Antigravity postures are difficult so use phasic bursts of movement • Move quickly to ends of range • Rest on ligaments, joint capsules, and bones
General Characteristics of Posture in Children with Hypotonia • Use wide BOS in both UEs and LEs • Move quickly to ends of range • Rest on ligaments, joint capsules, and bones
Prone • Postures: • Hyperextends neck and “rests” head back • Mouth is often open • Shoulder complex is often elevated to support head • Lower extremities are widely abducted and externally rotated • Movement: • Even neck extension is phasic…head may fall forward without control • No lateral weight shifts!!!!
Supine • Postures: • Prefers arms abducted and legs abducted • Body “melted” onto the floor • Movement: • Antigravity of extremities difficult • Sometimes “walks” extremities with hand movements • Can’t lift head against gravity • “Flings” extremities
Sitting • Postures: • Retains flexed spinal position with hyperextended head resting position • Sometimes looks like their chest “folds” in front • Uses UEs for support (hyperextended elbows) • May use feet as hands • Posteriorly tilted pelvis • BOS is very wide, knees flexed or extended
Sitting • Movement: • Keeps the COM in the middle of the BOS • Will pivot rather than rotate spine • Often transitions out of sitting in the sagittal plane with legs abducted
Mobility in Quadruped • Postures: • Hyperextension at the neck and elbows • UEs abducted • Hips and knees flexed greater than 90° • Hips abducted • Movement: • Moves extremities rapidly with longer periods of 4s support with extremities “locked” when possible • Much rather scoot on bottom!!!
Kneeling • Postures: • Support with UEs • Hips are abducted • Hips rest on feet or floor • Movement: • Difficult position to maintain • Will not transition to ½ kneel, pushes with legs at the same time to get to standing
Standing and Walking • Postures: • Still like hyperextended neck and kyphotic upper spine • UEs used to increase stiffness of trunk • Pelvis may be anteriorly or posteriorly tilted • Wide BOS in LEs • Knees hyperextended, out-toeing
Standing and Walking • Movement: • Legs may “fold” unexpectedly • Difficulty shifting weight laterally to unweight one leg for gait • Wide BOS and short steps make gait awkward and inefficient
M R Franjoine & M P Haynes + Domains- Dimensions NDT Enablement Classification Model of Health and Disability From: NDT Approach Theoretical Foundations & Principles of Clinical Practice, Table 2.1 pg. 82
M R Franjoine & M P Haynes + Domains- Dimensions NDT Enablement Classification Model of Health and Disability From: NDT Approach Theoretical Foundations & Principles of Clinical Practice, Table 2.1 pg. 82
Participation • Accepted by family…”good child” or “lazy child” • Often not accepted by peers due to latency of responses and communications • Sometimes problems safely accessing playgrounds and community centers
Treatment Strategies • Work upright whenever possible • Attend closely to alignment • Narrow the base of support • Emphasize weight shifts • May need to increase attention and/or arousal