Download
1 / 71
750 likes | 1.2k Views
Technique UKA. Lee Beom Koo Gachon university Gil Hospital. Pre-op measurement of tibia resection line & slope. Lateral joint line 을 기준으로 joint 에 parallel 하게 선을 긋고 그선에서 7mm 하방으로 선을 그은 후 그선 과 tibia medial plateau 와의 거리를 측정한 다 ( 대개 2-4 mm 이다 )

E N D
Technique UKA Lee Beom Koo Gachon university Gil Hospital
Pre-op measurement of tibia resection line & slope Lateral joint line을 기준으로 joint에 parallel 하게선을 긋고 그선에서 7mm하방으로 선을 그은 후 그선 과tibia medial plateau와의 거리를 측정한 다 ( 대개 2-4 mm이다) Lateral 사진을 보고sagittal slope측정하여 7 도 이하이면 natural slope로 ,cuttingline을 정하고 7도이상이면 slope를 7도 정도에 맞추어 자른 다
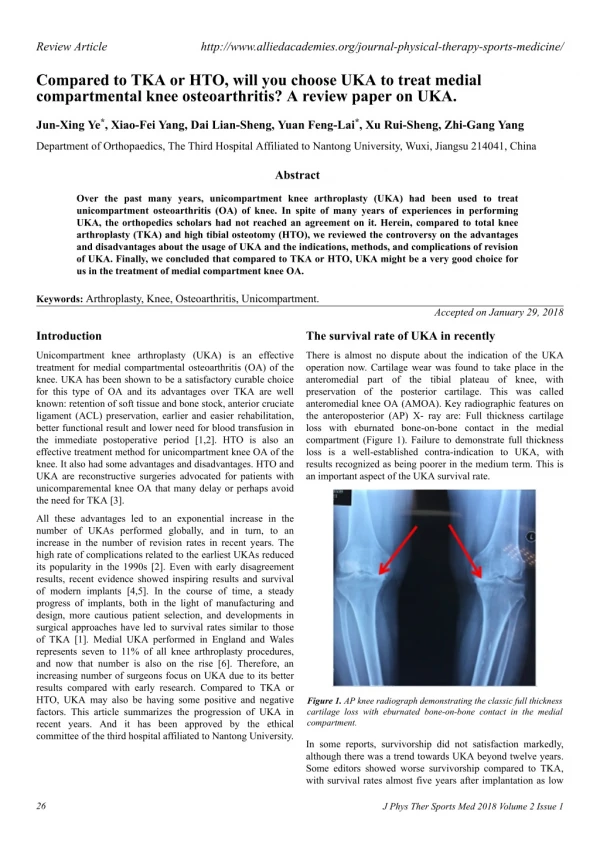
horizontal Tibial resection;depth • the depth of the tibial cut as conservative as possible to take advantage of the strength of the tibial cortex and the increased area of contact proximally • 2 to 4 mm off the deepest portion of the medial tibial plateau. • , 2-3 mm; oxford • . Scott Insall 4th edit Argenson, Jean-Noel A MD; Parratte, corr 464 Nov 2007 P32
Importanttechn in UKA • Our results seem to reflect those seen in registries confirming an earlier higher revision rate and highlight the technical issues of overstuffing the compartment, • The main issues in technique were overstuffing the medial compartment usually as a result of under resection of tibial bone and/or MCL attenuation • The desire for maximal bone preservation cannot supercede the need for adequte bone resection and varus resection on the tibial side aggravated this situation and must be avoided Initial Experience With the Oxford Unicompartmental Knee Arthroplasty Geoffrey F. Dervin MD, FRCSC, a, Chris Carruthers MD, FRCSCa, Robert J. Feibel MD, FRCSCa, Alan A. Giachino MD, FRCSCa, Paul R. Kim MD, FRCSCa and Peter R. Thurston MD, FR JA February 2011, Pages 192-197
Approach AM arthrotomy후 proximal tibia의medial soft tissue 를 elevation하는 데 deepMCL과 MCL tibia insertion중 proximal insertion은 elevate 한다 그후 The anterior part of medial meniscus 을 자르고 The medial spur도 rongeur and osteotome 으로 자른 다 MCLretractor 가 쉽게 들어갈 정도
Evaluation of joint While the patella is retracted. Resistance of ACL and state of cartilage of lateral & patellofemoral joint is inspected
Exposure of medial compartment patella를 retraction후 MCL 을MCL retractor로 retract하고 다리를 slight external rotation of leg 하면 전체적으로 좋은 시야가 나온 다
Adjustment and fixation of tibia guide Guide의 shaft를 tibia crest에 맞추어coronal alignment결정후 하나의 screw를 박아서 coronal alignment를 정한다 Guide의 center를 술전 tibiaaxis 만나는 곳에 둔다 . .
balancing After removal of the osteophytes, the varus deformity can be corrected. Scott Insall 4th edit
Adjustment and fixation of tibia guide Sagittal slope 를재고 distal 에서 guide를 올려서slope 를정한다 . The natural slope is preferred But slope greater than 7 is not recommended 수술전 계획 대로
Slope of tibia • usually between 5° and 7° of posterior slope • The natural slope is restored, but a posterior slope greater than 7 degrees is not recommended Argenson, Jean-Noel A MD; Parratte, corr 464 Nov 2007 P32 Scott Insall 4th edit
Posterior Slope of the Tibial Implant and the Outcome of Unicompartmental Knee Arthroplasty • Philippe Hernigou and Gerard Deschamps • J Bone Joint Surg Am. 2004;86:506-511
Horizontal cut • MCL retractor 로 MCL protection요하며. • 역시 너무 깊이 들어가 N_V 손상주지 않도록 조심 해야한다
The sagittal tibial cut 위치 ; The sagittal cutting line is marked at the medial edge of ACL Rotation; Sagittalcut line point toward the Femoral head in flexion ,akaki line medial femoral condyle wall방향 깊이; 너무 깊지 않게 , 깊으면 후에 tibia fx올수 있다
the direction of the sagittal cut • determined by the condyle itself • parallel to the wear pattern of the tibia • toward Femoral head in flexion (임홍철) • Having the patella not dislocated from the patellar groove is necessary for an appropriate tracking of component congruity. Scott Insall 4th edit Bobby로marking하면 좋다 이범구
Balance in extension After placement of sliding spacer block, the medial joint space should open up 1 or 2 mm when valgus stress is applied with the knee in full extension. It is very important to avoid overstuff & overcorrection
Balance in flexion , 2 to 3 mm laxity is suggested.in medial UKA after placing block For the balance in flexion, the thigh should be lifted with one arm to balance the flexion gap
Ideal balance ICL AAOS 2010 Richard A Berger P47
flexion gap balancing • performed by sliding a spacer block representing the thickness of the tibial component • To balance the flexion gap, the thigh should be lifted with one arm. • The block should slide backward with mild resistance. • 1 to 2 mm laxity is suggested.in medial UKA Scott Insall 4th edit
the proper thickness of the tibial component • . After medial compartment replacement, the medial joint space should open up 1 or 2 mm when valgus stress is applied with the knee in full extension. • . The deformity should not be overcorrected insall 4th edit Wolfgang FitzRichard D. Scott
Importanttechn in UKA • Our results seem to reflect those seen in registries confirming an earlier higher revision rate and highlight the technical issues of overstuffing the compartment, • The main issues in technique were overstuffing the medial compartment usually as a result of under resection of tibial bone and/or MCL attenuation • The desire for maximal bone preservation cannot supercede the need for adequte bone resection and varus resection on the tibial side aggravated this situation and must be avoided Initial Experience With the Oxford Unicompartmental Knee Arthroplasty Geoffrey F. Dervin MD, FRCSC, a, Chris Carruthers MD, FRCSCa, Robert J. Feibel MD, FRCSCa, Alan A. Giachino MD, FRCSCa, Paul R. Kim MD, FRCSCa and Peter R. Thurston MD, FR JA February 2011, Pages 192-197
If the flexion gap is too tight;first step 종종 pre-optibia slope가 7도 이상이나 tibia 를 slope를 7도로 주고 하면 flexion gap이 tight해진 다 If the flexion gap is too tight , cartilage or bone should be removed from the posterior condyle offemur with rasp or saw
If the flexion gap is too tight;2nd step or The slope should be slightly increased
Marking of femoral rotation line Next step for the Marking of femoral rotation line the center of the tibial spacer block is marked with a Bovie on the femoral condyle in different positions It should not be judged while the patella is everted or perpendicular line to the cut tibia bone can be chosen
Distal femoral cut the distal femoral cutting guide is slided in extension and fixed with two pin and resected . The knee should be flexed 5 if the resected posterior slope of tibia is 5 to avoid hyperextension. shim can be used to manage the bone defect. Distal cut가 flex해지면 flex gap이 tight해진다 Tilt안 되게 자른 다 자른 골의 두께 를 측 정, shim이 위로 안 가게 check
Slope of distal femur cutting • For example, for a 5-degree tibia slope • the knee should be held in 5 degrees of flexion to fix the distal femoral cutting block. • Because If the distal femoral cutting block is pinned in full extension, the knee will hyperextend 5 degrees, as determined by the tibial slope Scott Insall 4th edit
The entrance hole of the distal femur • centered above the roof of the intercondylar notch. • often requires bringing the knee to lower degrees of flexion; otherwise, in flexion, the unyielding patella might induce incorrect alignment of the intramedullary guide Argenson, Jean-Noel A MD; Parratte, corr 464 Nov 2007 P32
Scuderi Insall 4th edit The drilling of the femoral medullary canal through a short incision often requires bringing the knee to lower degrees of flexion; otherwise, in flexion, the patella might induce incorrect alignment of the intramedullary guide.
the distal femoral cut ;Angle • calculated on the full weightbearing view • the angle between the anatomic and mechanical axis is chosen • This angle is usually 4° to 6°
The amount of bone resected The amount of bone resected ; corresponds to the femoral prosthesis thickness Scuderi Insall 4th edit the deeper resection (line A) results in less valgus than line B (3 degrees versus 5 degrees). This also allows for more space in full extension For valgus knees, it is often necessary to use a more proximal distal femoral cut
The Extramedullary Spacer Block Technique Figure 82-15 A, After tibial resection the gap is checked with a spacer block. B, The appropriate spacer block is inserted into the joint space. C, The spacer block and distal cutting guide assembly are shown. D, The distal cutting guide is secured to the distal femur. E, Alignment is confirmed with the appropriate block and rod. Scuderi Insall 4th edit
Finishing cutting guide placement Femur finishing guide is inserted in 90 degree flexion .
Finishing cut ;Size If the size is proper, 1 to 2 mm of exposed bone . At the anterior edge
The anterior extent of the weightbearing surface • defined by the junction between the eburnated bone of the femoral condyle and the intact cartilage remaining in the trochlear groove.
Finishing cut ;Size There should be 1 to 2 mm of exposed bone along the anterior edge of the guide. The leading edge of the femoral component must be countersunk into this junction to prevent patellar impingement during flexion of the knee If the finishing guide appears to be between sizes, it is preferable to pick the smaller size. Scuderi Insall 4th edit
Mediolateral dimension For the correct mediolateral position, The guide should be placed in the center of the femoral condyle,mediolaterally
Rotation femoral rotation may follow the previously Marked rotation line or This guide should also be rotationally set so that the posterior cutting surface of femoral condyle is parallel to the resected tibia
Finishing cut ;To assess the amount of external rotation,. • the center of the tibial trial is marked with a Bovie on the femoral condyle in different positions (90, 60, 30, 0 degrees).. • The femoral prosthesis should be only slightly externally rotated • External rotation of more than 5 degrees is not recommended so that the possibility of edge loading is minimized. Scott Insall 4th edit
Finishing cut; rotation .This guide should also be rotationally set so that the posterior surface is parallel to the resected tibia Guide를 tibia spacer넣고 그위에 finishing guide넣으면 편할 듯 이범구 Scuderi Insall 4th edit
Fixation of finishing guide Posterior & Champer cut Finishing guide is fixed with two screw. at the Anterior margin of guide, bone is gouged slightly to accept the curved prosthesis While the MCL is protected with MCL retractor placed at femoral side, the posterior femur is resected and after anterior and posterior chamfer cut , two femoral peg hole is drilled
Posterior condyle resection • . The posterior condylar bone should be resected to at least the thickness of the metallic implant. • It is better to resect slightly too much of the posterior condyle than too little to avoid making the components too tight in flexion Scott Insall 4th edit
removal of any posterior osteophytes • Once the posterior cut has been made and the cutting guide removed, removal of any posterior osteophytes is necessary using a curved osteotome to increase the range of flexion and avoid any posterior impingement with the polyethylene in high flexion Scott Insall 4th edit
The femoral component should be placed • in the center of the mediolateral dimension of the femoral condyle,. when the knee is extended • . The femoral component should extend far enough anteriorly to cover the weightbearing surface that comes in contact with the tibia in full extension. • the articulating surfaces of the two components are rotationally congruent during weightbearing . in full extension. • It should not be judged while the knee is flexed and the patella is everted. Scott Insall 4th edit
Post. Condyle trimming to avoid impingement posteriorly Post. Condyle trimming to avoid impingement posteriorly
The final preparation of the tibia;exposure The leg is externally exposed, while the MCL is retracted to expose the whole medial compartment
The size of the tibial tray Size는 AP 길이를 보고 결정해야한다 종종 ACL 보다떨어져서 sagittal cut하는데 medial크기가 작아진 다 그후 coronal plane으로크기 정하면 AP상 적은 크기가 들어가고 cortical support가 안 된다; tibia plate가 cancelleous bone에만 걸치므로 조기collapse가 온 다