Download
1 / 52
520 likes | 531 Views
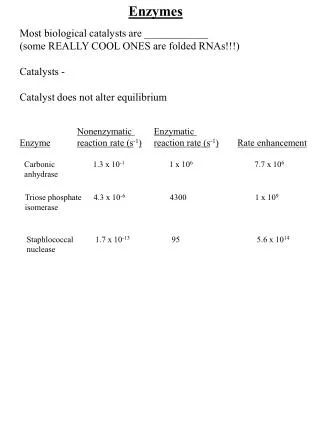
Enzymes. Clinical significance & Methods. Measurements of enzymes. in serum within a tissue enzymes as markers of disease, Injury to tissue releases cellular substances that can be used as plasma markers of tissue damage. enzyme release is highly specific for cell death in some settings.

E N D
Enzymes Clinical significance & Methods
Measurements of enzymes • in serum • within a tissue • enzymes as markers of disease, • Injury to tissue releases cellular substances that can be used as plasma markers of tissue damage. • enzyme release is highly specific for cell death in some settings.
Some enzymes are predominantly found in the specialized tissue • while others, more widely distributed, have tissue specific isoenzymes or isoforms • The timing of the enzyme's diagnostic window • early indicators • late indicators • Several enzymes have diagnostic utility
Overlap occurs for some enzymes • may be used for investigating disease in several organs.
Enzymes of clinical interest MUSCLE ENZYMES • More commonly measured • CK, LD • CK; adenosine triphosphate: creatine N-phosphotransferase
Inhibitors • excess Mg2+ • Many metal ions, such as Mn2+ , Ca2+ , Zn2+ ,Cu2+ • sulfhydryl-binding reagents • Iodoacetate
CK is a dimer (B and M) • the products of loci on chromosomes 14 and 19, respectively. • BB (or CK-1), MB (or CK-2), and MM (or CK-3). • numbered on the basis of their electrophoretic mobility, with the most anodal form receiving the lowest number. • The distribution of these isoenzymes in the various tissues
Serum CK activity is subject to a number of physiological variations. • Sex, age, muscle mass, physical activity, and race all interact to affect serum activities
Clinical Significance • Serum CK activity is greatly elevated in all types of muscular dystrophy. • may be increased long before the disease is clinically apparent. • Serum CK activity characteristically falls as patients get older and as the mass of functioning muscle diminishes with the progression of the disease.
Long time Physical inactivity reduce serum CK • Skeletal muscle that is diseased or damaged (fetal reversion) • Renal failure , increase CK • Serum CK activity demonstrates an inverse relationship with thyroid activity. • Following a myocardial infarction • MB isoenzyme
The assay of CK activity • Coupled enzyme methods NADP+ to NADPH, monitored spectrophotometrically.
CK activity in serum is relatively unstable and is rapidly lost during storage. • Average stabilities are less than 8 hours at room temperature, 48 hours at 4°C, and 1 month at -20°C. • Methods for the Separation & Quantification of CK Isoenzymes • Electrophoresis & various immunological methods.
Enzymes of clinical interest • Widely used enzymes • Aspartate aminotransferases (AST) • Alanine aminotransferases (ALT) • ALP
The aminotransferases • The aminotransferases • catalyze the interconversion of amino acids to 2-oxo-acids • L-aspartate:2-oxoglutarate aminotransferase;AST • L-alanine:2-oxoglutarate aminotransferase; ALT
Pyridoxal-5'-phosphate ↔ pyridoxamine-5' –phosphate • Both the coenzyme-deficient apoenzymes and the holoenzymes may be present in serum. • All factors affecting the rate of reaction must be optimized and controlled
Clinical Significance • Liver disease is the most important cause of increased transaminase activity in serum. • In most types of liver disease, ALT activity is higher than that of AST; • exceptions • alcoholic hepatitis, hepatic cirrhosis, and liver neoplasia. • elevated even before the clinical signs and symptoms of disease
Peak values of transaminase activity occur between the 7th and 12th days • Medications • nonsteroidalantiinflammatory drugs, antibiotics. • ALT is the more liver-specific enzyme. • elevations of ALT activity persist longer than do those of AST activity.
After AMI, increased AST activity appears in serum • AST activity also is increased in some types of muscle diseases • Also serum CK • Mitochondrial AST (m-AST) activity • extensive liver cell degeneration and necrosis. • the ratio between m-AST and total AST activities • typical of alcoholic hepatitis
The increased AST activity might reflect decreased clearance • Macro-AST
Measurement of Transaminase Activity • coupling the transaminase reactions to specific dehydrogenase reactions. Pyruvate formed in the ALT reaction is reduced to lactate by LD.
The change in absorbance per minute (ΔAlmin) is proportional to the micromoles of NADH oxidized and in turn to micromoles of substrate transformed per minute. • AST activity in serum is stable for up to 48 hours at 4°C. • ALT stability is better maintained at -70°C.
Reference Intervals • AST; 31 U/L for women and 35 U/L for men • Methods for the Separation & Quantification of AST Isoenzymes • electrophoresis, selective inhibition, and immunoassays. • anionic (cytoplasmic AST) and a cationic band (m-AST)
m-AST (healthy individuals ) • About 5% to I0% of the activity of total AST in serum • 3.0 U/L.
ALKALINE PHOSPHATASE • ALP • Orthophosphoric monoester phosphohydrolase • alkaline optimum • hydrolysis of a large variety of naturally occurring and synthetic substrates • ALP activity is present in most organs of the body • especially associated with membranes and cell surfaces • In the mucosa of the small intestine and proximal convoluted tubules of the kidney, in bone (osteoblasts), liver, & placenta
Metabolic function • Lipid transport in the intestine • Calcification process in bone • ALP exists in multiple forms
activators of the enzyme, • divalent ions, Zn2+ • Inhibitors • Phosphate, cyanide ions,… • The ALP activity in the sera of healthy adults • Liver • Skeleton
Clinical Significance • Common causes of elevation • Liver • Hepatobiliary disease • bone • Bone disease associated with increased osteoblastic activity • Carcinoplacentalisoenzymes • derepression of the placental ALP gene • non placental isoenzymes • Modified forms of ALP
Determination of Alkaline Phosphatase Activity • The rate of formation of 4-NP at 405 nm is monitored
Determination of Alkaline Phosphatase Activity • Serum or heparinized plasma, free of hemolysis, should be used. • Freshly collected serum or up to 4 hours RT* • Frozen specimens; ALP activity increases • kept at room temperature for 18 to 24 before assay *Room temperature
Reference Intervals ALP activities in serum vary with age.
Methods for the Separation and Quantification ofAlkaline PhosphataseIsoenzymes • Assays for ALP isoenzymes are needed when: • the source of an elevated ALP in serum is not obvious • to monitor the disease activity and the effect of appropriate therapies • Electrophoretic mobility • Stability to denaturation by heat or chemicals • Response to the presence of selected Inhibitors
anodal mobility, • The liver, most rapidly • Bone ALP, slightly lower • Intestinal ALP • Placental isoenzyme • Discrete band overlying the diffuse bone fraction • Improvement of electrophoretic separation • treated briefly with neuraminidase • Electrophoresis in the presence of wheat germ lectin
Placental ALP is heat stable • 65°C for 30 min • Other evidences • eg ;measurement of GGT • Immunological methods • Intestinal or placental ALPs.
Acid Phosphatase (ACP) • Include all phosphatases • that hydrolyze phosphate esters with an optimum pH of less than 7.0. • Produced by • Primarily, prostate gland, • also found in • erythrocytes, platelets, leukocytes, bone marrow, bone, liver, spleen, kidney, and intestine.
Acid Phosphatase (ACP) • ACP is present in • Lysosomes, • Extra lysosomal • The lysosomal and prostatic enzymes • strongly inhibited by D-tartrate ions, • the erythrocyte and bone isoenzymes • are not inhibited.
Acid Phosphatase (ACP) • Normal serum ACP • The majority of the normally low ACP activity of (unhemolyzed) serum is of a • Tartrate-resistant type (TR-ACP) • Probably originates mainly in osteoclasts. • Increased • Physiologically in growing children • Pathologically in conditions of increased osteolysis and bone remodeling. • High concentrations of TR-ACP in serum • Reflect increased osteoclastic activity, whether appropriate as in normal bone growth, or damaging
The only nonbonecondition • Gaucher'sdisease • of spleen, a lysosomal storage disorder, • elevated activities of TR-ACP are found in serum, • abnormal macrophages in spleen and other tissues, overexpress ACP
Acid Phosphatase (ACP) • ACP-determining genes • At least four have been identified and mapped. • ACPs are labile • more than 30% of the ACP activity may be lost in 3 hours at room temperature. • Acidification of the serum • specimen to a pH below 6.5 aids in stabilizing the enzyme activity.
Acid Phosphatase • Prostatic acid phosphatase (PAP), • an optimum pH of 5 to 6, • very labile at a pH of greater than 7.0 • very labile at temperature greater than 37°C. • Distinguished from other acid phosphatases by • Using tartrate, • Strongly inhibits the prostatic form. • Select substrates that are more specific for PAP • thymolphthalein monophosphate and β-naphtholphosphate. • Hydrolyzed by PAP much more quickly
Acid Phosphatase • The clinical use of PAP • as a screening tool for prostate cancer. • to help stage prostate cancer, • to correlate with the prognosis of the disease, • to monitor therapy. • Elevated serum PAP may be seen in • malignant conditions, • osteogenicsarcoma, multiple myeloma, and bone metastases of other cancers. • in some benign conditions, • Osteoporosis, benign prostatic hyperplasia and hyperparathyroidism.
Acid Phosphatase • The clinical use of PAP • has been replaced by PSA • PAP is not as sensitive as PSA for screening or for detection of early cancer. • restricted to confirmation of metastatic prostate cancer and staging of prostate cancer. • Currently the method of choice for PAP • Measurement of enzymatic activity.
Acid Phosphatase • Measurement of ACP • Methods • Continuous-monitoring methods of ACP activity • Immunological methods • Principle: • Thymolphthalein monophosphate is hydrolyzed by prostatic ACP at pH 5.4 and 37°C. • The reaction stopped after 30 min by addition of NaOH-Na2CO3 solution • This develops the alkaline color of the liberated Thymolphthalein • Measured at 595 nm
Acid Phosphatase • Specimens: • Serum should be immediately separated from erythrocytes and stabilized by the addition of acetic acid to lower the pH to 5.4 • Under these conditions, ACP activity is maintained at room temperature for several hours, • for up to a week if the serum is refrigerated, and for 4 months if stored at -20°C.