Download
1 / 65
650 likes | 791 Views
Risk Assessment for Esophageal Adenocarcinoma. June 2014 Thomas Vaughan Fred Hutchinson Cancer Research Center. Two Distinct Cancers. Incidence of Esophageal Adenocarcinoma. Arithmetic. Log. WM. BM. WF. BF. NCI SEER*Stat Database: 9 Registries released April 2013.

E N D
Risk AssessmentforEsophageal Adenocarcinoma June 2014 Thomas VaughanFred Hutchinson Cancer Research Center
Incidence of Esophageal Adenocarcinoma Arithmetic Log WM BM WF BF NCI SEER*Stat Database: 9 Registries released April 2013
Natural History of EA Normal 20%Chronic Reflux (GERD) 10% Metaplasia (Barrett’s*) HG Dysplasia 0.2 - 0.5% annualAdenocarcinoma *2-4 M persons in U.S. with Barrett’s
Metaplastic Epithelium Wild & Hardie, Nat Can Rev, 2003
Surveillance Rationale Survival Cancer detected during surveillance Local Distant SEER Limited Use Data, 9 registries, April 2007
Male Sex 8.0 3 - 4 2 Hardikar, PLoS ONE 2013; Edelstein, AJG 2009; Corley, Gastro 2007
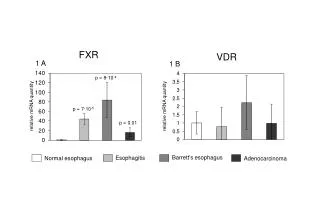
Genetic Contribution to Risk h2g = 25% (p~10-7) h2g = 35% (p~10-9) minimal ? • Significant genetic contribution to BE and EA • The many common genes contributing to these disease are largely shared between EA and BE Ek, JNCI 2013
Aspirin/NSAIDs 0.6 – 0.7 ~ 1 ~ 0.5 Liao, Gastro 2012; Vaughan, Lancet Oncology 2005
Precision Prevention ? Reid et al, Nat Can Rev, 2010
Primary Care SettingVery Low Risk • History/Physical (lifestyle, family history, obesity) • Low cost clinical screening based on • Blood (e.g., H pylori, telomeres, inflammatory cytokines) • Non-endoscopic cytology markers (e.g., Cytosponge) • Risk prediction tool for education/referral
Secondary Care SettingLow Risk • Reproducible tissue-based markers • Safe interventions (e.g., lifestyle) • Secondary care risk model to guide surveillance and interventions
Secondary Care SettingModerate Risk • Cost-effective surveillance protocol • Cost-effective interventions (e.g., chemoprevention) • Stratification into highest risk category
Discrimination and calibration of risk model for BE among persons with reflux symptoms. - Thrift, et al. Cancer Prevention Research 2012
“Cytosponge” • Non-endoscopic collection of esophageal epithelial cells
Risk PredictionBarrett’s –> EA • Goal: Develop risk prediction models based on sets of variables available in different contexts (increasing cost) 1. Questionnaire based e.g., age, sex, reflux sx, obesity measures, smoking history, nsaid use 2. Adding blood measures e.g., CRP, leptin, insulin, metabolite panel 3. Adding clinical endoscopy data e.g., Barrett’s segment length 4. Adding somatic genetic abnormalities (biopsy-based) e.g., specific mutations (p53) or genome-wide abnormalities • Steps: Impute missing data (50 datasets) Fit model using backward stepwise regression (also forward) with a threshold for staying in the model of p<0.2 • Model is fit on each imputation and Rubin’s rules are used to combine the estimated coefficients and variances across imputations.
Risk PredictionBarrett’s –> EA • AUC • Naïve AUC is calculated as average AUC of final model across imputations • “adjusted” AUC is based on 100-fold cross-validation with a 2/3rds vs 1/3rds training/test split using the same backward stepwise regression procedure • Calibration of model: still working on this but same ideas as above • Above steps repeated for different contexts. Thrift, Janes, Onstad, et al., in process
Challenges & Discussion Points • Defining priorities • What context deserves top priority? • What data are needed/available to address each context? • Biomarkers & other unproven predictors • Confronting limited data resources • Small numbers for some contexts • Missing data • How to validate in consortium setting where we already have most cases (e.g., rare disease) • Implementing decision aids • Most value for physicians • Most value for patients/population
Comparison of multiple cardiovascular risk scores Rebekah Young rlyoung@uw.edu June 11, 2014
Cardiovascular Risk Scores • A risk assessment tool to predict a person's chance of having a heart-related event over some period of time (usually 10 years) • Risk scores are used by physicians to initiate discussion of preventive medication
1. Points-based TC 2. Points-based LDL 3. Equation-based TC 4. Equation-based LDL
Framingham Risk Scores Age: 59 Total cholesterol (TC): 148 High-density lipoprotein (HDL): 35 Systolic blood pressure (SBP): 120 Antihypertensive medication use: Yes Smoker: Former Family history of heart disease(FH): No Diabetes (DM): No
Framingham Risk Scores Age: 59 Total cholesterol (TC): 148 High-density lipoprotein (HDL): 35 Systolic blood pressure (SBP): 120 Antihypertensive medication use: Yes Smoker: Former Family history of heart disease(FH): No Diabetes (DM): No
Framingham Risk Scores Age: 59 Total cholesterol (TC): 148 High-density lipoprotein (HDL): 35 Systolic blood pressure (SBP): 120 Antihypertensive medication use: Yes Smoker: Former Family history of heart disease(FH): No Diabetes (DM): No
Framingham Risk Scores Age: 59 Total cholesterol (TC): 148 High-density lipoprotein (HDL): 35 Systolic blood pressure (SBP): 120 Antihypertensive medication use: Yes Smoker: Former Family history of heart disease(FH): No Diabetes (DM): No
Framingham Risk Scores Age: 59 Total cholesterol (TC): 148 High-density lipoprotein (HDL): 35 Systolic blood pressure (SBP): 120 Antihypertensive medication use: Yes Smoker: Former Family history of heart disease(FH): No Diabetes (DM): No
Multiple Cardiovascular Risk Scores • A cautionary tale about using “TheFramingham risk score” • Different target populations (e.g.,diabetics, different age ranges) • Different endpoints • Variation within same endpoint • Overlap in the compositeFRS-98-TC-Pt: Angina, MI, CHD death, coronary insufficiencyFRS-ATP3-Eq: MI, CHD death • Issue with online calculators
Multiple Cardiovascular Risk Scores • A cautionary tale about using “TheFramingham risk score” • Different target populations (e.g.,diabetics, different age ranges) • Different endpoints • Variation within same endpoint • Overlap in the compositeFRS-98-TC-Pt: Angina, MI, CHD death, coronary insufficiencyFRS-ATP3-Eq: MI, CHD death • Issue with online calculators