Download
1 / 22
290 likes | 516 Views
OTITIS MEDIA. Definition: inflammation of the middle ear Very common in children but can occur in any age. Subtypes of OM. Acute otitis media (AOM) Otitis media with effusion (OME) Chronic suppurative otitis media (CSOM) Adhesive otitis media.

E N D
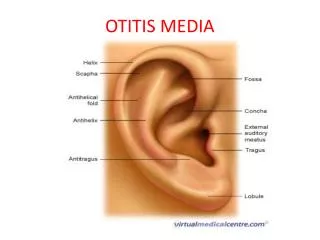
OTITIS MEDIA • Definition: inflammation of the middle ear • Very common in children but can occur in any age
Subtypes of OM • Acute otitis media (AOM) • Otitis media with effusion (OME) • Chronic suppurative otitis media (CSOM) • Adhesive otitis media
Acute otitis media (AOM) develops suddely due to a (viral or bacterial) upper respiratory infection with blockage of the Eustachian tube. • The most common bacteria found in this case are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
Otitis media with effusion (OME), also called serous or secretory otitis media (SOM) or GLUE ear. • it is simply a collection of fluid that occurs within the middle ear space due to the negative pressure produced by altered Eustachian tube function. • This can occur purely from a viral URI, with no pain or bacterial infection, or it can precede and follow acute bacterial otitis media.
Fluid in the middle ear sometimes causes conductive hearing impairment,. Over weeks and months, middle ear fluid can become very thick and glue-like (thus the name glue ear).
Chronic suppurative otitis media involves a perforation (hole) in the tympanic membrane and active bacterial infection within the middle ear space for several weeks or more. • There may be enough pus that it drains to the outside of the ear (otorrhea), or the purulence may be minimal enough to only be seen on examination using a binocular microscope. • This disease is much more common in persons with poor Eustachian tube function. • Hearing impairment often accompanies this disease.
Adhesive otitis media – if fluid is present within the ear for a protracted period, the tympanic membrane retracts and will adhesive to the middle ear, and adhesive otitis media may develop.
Causative organisms • Streptococcus pneumoniae • Haemophilus influenzae • Moraxella catarrhalis • Group A Streptococcus • Staph. aureus • Pseudomonas aeruginosa • RSV
RISK FACTORS • Upper Respiratory Infections • Eustachian tube malformations • Allergies • Craniofacial abnormalities (cleft palate) • Smoking • Cholesteatoma
Pathophysioloy • This problem mainly deals with Eustachian tube dysfunction. • Otitis Media usually follows an URI in which there is edema of the eustacian tube, leading to blockage. Stasis of these middle ear secretions lead to infection and irritation • Other factors: allergic rhinitis, nasal polyps, adenoidal hypertrophy
Causative factors (mainly URI) • Edema in the Eustachian tube • Blockage in the Eustachian tube • Stasis of middle ear secretions • Irritation • Inflammation • Signs and symptoms
SIGNS & SYMPTOMS • Otalgia – throbbing pain • Otorrhea • Headache • Fever • Irritability • Loss of appetite • Vomiting • Hearing loss • Tinnitus • Vertigo
Diagnostic measures • History collection • Physical examination • Pneumatic otoscopy – gold standard mearsure • Tympanometry • Reflectometry • Mastoid x- rays
The classic description for Otitis Media is an erythematic, opaque, bulging tympanic membrane • Pneumatic Otoscopy: decreased tympanic membrane mobility • Spectral Gradient Acoustic Reflectometry: measures the condition of the middle ear by assessing the response of the TM to a sound stimulus. Equivalent to tympanometry for diagnosing middle ear effusions
Management • Antibiotics – assess for allergies and hypersensitivity reactions, inform not to miss any doses • Analgesics – do not drive after taking codeine, inform to take increase fluid • Antihistamines - chlorpheniramine • Decongestants - pseudoephedrine
Analgesics – acetaminophen, ibuprofen • Amoxicillin (drug of choice): 20-40 mg/kg/day tid for 10-14 days or, • Augmentin: 45 mg/kg/day bid for 10-14 days • Auralgan: analgesic/adjunct for ear pain 2-4 drops tid
2nd Line Treatment Regimen • Cefzil (cefprozil) • Pediazole ( erythromycin/sulfisoxazole) • Bactrim (trimethoprim/sulfamethoxazole • These medications are used as secondary agents if the primary antibiotic has failed after 10 days and the symptoms persists.
Surgical management • Tympanocentesis & myringotomy • Tympanoplasty with mastoidectomy • Tympano – ossiculoplasty • Resection of the cholesteatoma
Tympanocentesis & myringotomy: • involves puncturing the tympanic membrane and aspirating middle ear fluid to relieve pressure. Only used if the primary and secondary line treatment fail.
COMPLICATIONS • Hearing loss: conductive, sensorineural, mixed) • Acute mastoiditis • Chronic perforation of the TM • Tympanosclerosis • Cholesteatoma • Chronic suppurative OM • Facial nerve paralysis
Complications • Intracranial complications • Bacterial meningitis • Epidural abscess • Brain abscess • Hydrocephalus
Prevention • Most common in children so adequate breast feeding should be given • OM follows a respiratory tract infection, so treat the respiratory infections as soon as possible • Day care centers is considered as a source, so proper follow up should be maintained. • Health awareness programme in day care centers, schools can be helpful