Download
1 / 39
400 likes | 603 Views
The Cochrane Collaboration’s Prioritization Approaches. Lorne Becker: Co-Chair, Cochrane Collaboration Steering Group US Cochrane Center Conference on Priority Setting for Systematic Reviews July 10 2008, Baltimore, USA. Outline of presentation. Dangers & difficulties in prioritization

E N D
The Cochrane Collaboration’sPrioritization Approaches Lorne Becker: Co-Chair, Cochrane Collaboration Steering Group US Cochrane Center Conference on Priority Setting for Systematic Reviews July 10 2008, Baltimore, USA
Outline of presentation • Dangers & difficulties in prioritization • Cochrane approaches to prioritization • Individual Cochrane “entities” • Organization-wide
Dangers and difficulties • Is prioritization compatible with the Cochrane way of doing things? • What are the opportunity costs? • Whose priorities would we follow?
How Cochrane Review Topics are Chosen • Curiosity driven • Investigator-initiated • Peer-reviewed
Cochrane Decision Making • Primarily bottom up • Authors’ interests • Scope of editorial group (CRG) • Minimally top down • Methods • Procedures • Updating
10 Cochrane Principles #2 - Building on the enthusiasm of individuals, - by involving and supporting people of different skills and backgrounds.
Could Prioritization Help Focus Collaboration Efforts? • Prioritization helps decide what not to do • Cochrane aim is to build a comprehensive database of reviews • What to do first
Who Are Our Stakeholders? Consumers? Clinicians? Spouses, Families, Caregivers?
Who Are Our Stakeholders? Policy Makers? Consumers? Clinicians? Guideline Writers? Spouses, Families, Caregivers? Advocacy Groups?
Who Are Our Stakeholders? Policy Makers? Consumers? Clinicians? Guideline Writers? Researchers? Spouses, Families, Caregivers? Methodologists? Advocacy Groups?
Who Are Our Stakeholders? Of Research? Funders? Policy Makers? Consumers? Clinicians? Guideline Writers? Researchers? Spouses, Families, Caregivers? Methodologists? Of Health Care? Advocacy Groups? Of Reviews?
Priority setting • Be sure not to miss important perspectives or stakeholders
How would these Cochrane reviews have been prioritized? • Routine perineal shaving on admission in labor • Episiotomy for vaginal birth
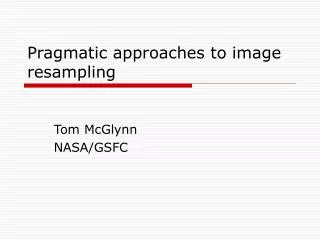
Diabetes Prevalence www.WorldMapper.org
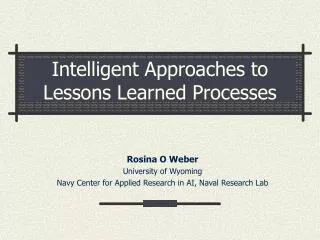
Tuberculosis Prevalence www.WorldMapper.org
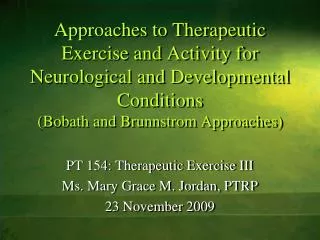
HIV Prevalence www.WorldMapper.org
Women Smokers www.WorldMapper.org
Until 2006 No central prioritization process Each of the 52 editorial groups responsible for setting its own priorities Variety of approaches Cochrane Prioritization Processes
Skin Group • 21 titles proposed for development • Resources allow only 6 • Vote by Skin Group Members vote to rank titles in order of priority. • Authors • Editors • Peer reviewers • Consumers
Skin Group – results of prioritisation • Sentinel node biopsy followed by elective node dissection for early malignant melanoma. • Maintenance treatment for chronic plaque type psoriasis. • Topical corticosteroids for atopic eczema. • Interventions for erosive lichen planus. • Interventions for mycosis fungoides. • Concomitant hyperthermia and radiation for recurrent or metastatic malignant melanoma.
Renal Group • Examination of Trial Register by staff • Identification of important studies • Group studies into broad topical areas • Split each topic into several manageable reviews. • Post list of priority topics on web site
Infectious Diseases Group • Interplay of 3 criteria • Importance of the topic • Number of trials (0, 1, 2+) • Availability of experienced author team
Importance – Cochrane ID Group 1 – Strategic Importance Known interest from funders, policy makers or other key stakeholders 2 – Potentially Important WHO Millennium Development Goals Health in Developing Countries 3 – Minimal relevance to MDGs
Health Promotion & Public Health Group • Taskforce of advisors from global health organizations • Identified “policy-urgent topics” • Literature review for existing SRs • List of potential review topics to fill the gaps • Prioritization of the list by the Advisor taskforce • Dissemination throughout the Collaboration to relevant editorial groups • Formation of a Health Promotion & Public Health editorial group J Epidemiol Community Health 2005;59:193–197
Steering Group Perspective • A key recommendation of the 2006 Steering Group review • Half day session at 2006 mid year meetings • £100,000 to fund prioritization projects
Cochrane Prioritization Projects • Top down vs. Bottom up • Call for proposals from Cochrane entities • Opportunity Costs • £100,000 from central Cochrane funds • Whose Priorities? • Up to applicant entities to decide
Collaboration between a Cochrane Review Group and a Cochrane Field • Condition: • Hip fracture rehabilitation • Cochrane Entities: • Bone, Joint and Muscle Trauma Review Group • Health Care of Older People Field • Whose Priorities? • Members of the CRG and the Field
A patient-professional partnership approach • Condition: - Incontinence • Cochrane Entities: • Cochrane Incontinence Review Group • Collaborators: • The James Lind Alliance • a UK-based patient support charity • Whose Priorities? • 30 patient and professional advocacy groups
Using practice guidelines to determine review priorities • Condition: • Eye and Vision Disorders • Cochrane Entities: • US Cochrane Centre • Eyes and Vision Review Group • Whose Priorities? • International clinical experts
Prioritisation of Cochrane reviews for consumers and the public • Condition: • Any with a current Cochrane Review • Cochrane Entities: • Cochrane Consumer Network • Whose Priorities? • Consumers in low and middle income countries • Identify Reviews most in need of updating
Reducing the know-do gap in low and middle income countries • Condition: • Relevant to most disadvantaged in LMICs • Cochrane Entities: • Health Equity Field • Health Promotion & Public Health Field • Developing Countries Network • EPOC Review Group • Whose Priorities? • Experts on health of the disadvantaged in LMICs • Similar methodology to HPPH group
Conclusion Prioritization is seen as desirable But there are potential questions & difficulties The Collaboration is proceeding deliberately And hoping to learn from our experiences