Download
1 / 24
250 likes | 582 Views
DMI 56 Skeletal System Ch 4-Part 2 . Marilyn Rose RT, RDMS. Fibrous Dysplasia Ischemic Necrosis of Bone Benign Bone Tumors Malignant Bone Tumors Bone Mets Fractures Fractures/ dislocations of Spine Herniation of Intervertebral Disks Scoliosis Spondylolysis and Spondylolisthesis.

E N D
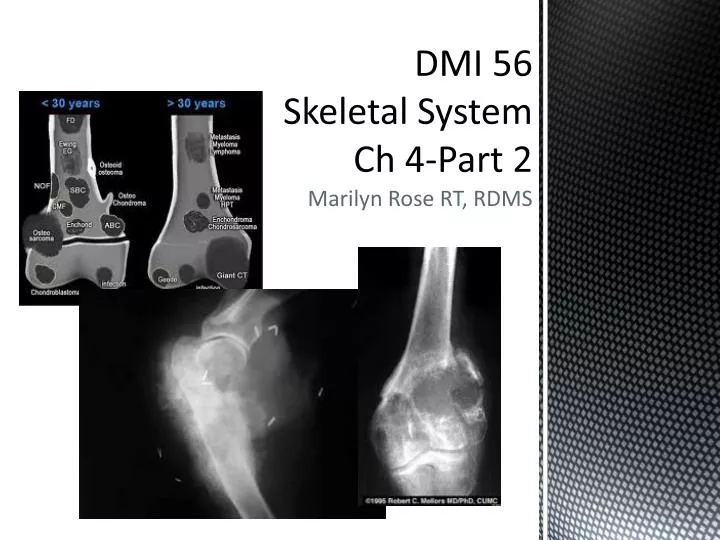
DMI 56Skeletal SystemCh 4-Part 2 Marilyn Rose RT, RDMS
Fibrous Dysplasia • Ischemic Necrosis of Bone • Benign Bone Tumors • Malignant Bone Tumors • Bone Mets • Fractures • Fractures/ dislocations of Spine • Herniation of Intervertebral Disks • Scoliosis • Spondylolysis and Spondylolisthesis Outline- Part 2
Begins during childhood • Characterized by proliferation of fibrous tissue w/in medullary cavity • Causes trabecular loss and widening of bone • Monostotic= Single bone • Adults= Extremity most common • Polyostotic- children –girls- involves ½ skeleton with 25% of skull • Primarily the long bones • Especially femur, tibia, • Ribs and facial bones • Radiographic- • radiolucent area- can be radiolucent or homogenous ground glass • Sclerosis may cross cyst lesion giving it a multilocular appearance • Bone locally expands – balloon • Pathologic fx are common • Bowed or deformed bones • CT is best to compliment xray Fibrous dysplasia
Loss of blood supply • Varied conditions • Thrombosis • Vaculites • Disease of surrounding bone • Single or repeated episodes of trauma • Acute trauma (fx /dislocation) • Steroid tx • Cushing's dx • Hemolytic anemia • Sickle cell • Chronic alcoholism • Chronic pancreatitis • Gaucher’sdz • Rad tx • Caisson’s dz= underwater diving= Bends Ischemic necrosis of bone Radiographic- femoral head most common site for ischemic necrosis Initially denser that adjacent Radiolucent subcortical band= crescent sign= fx line Fragmentation / absorption of dead bone proliferation of granulation tissue revascularization and production of new bone produce a patter of lytic/ sclerotic areas flattening of femoral head perostial new bone formation Uneven weight bearing and secondary DJD >kVp Radionucleotide bone scan most sensitive
Osteochondroma • Enchondroma • Giant cell tumor • Osteoma • Osteoid osteomas • Simple bone cysts • Aneurysmal bone cyst Benign Bone tumors
Exostosis • Benign projection of bone with cartilaginous cap • Arises in childhood • Especially around the knee • Exostosis occurs in epiphyseal plate • If cartilage cap is thick- risk of malignancy- chondrosarcoma or osteosarcoma • US can evaluate the cap thickness • Hereditary form- > risk of malignancy • Xray preferred method • MRI is best for cartilage cap and rule of malignancy osreochondroma
Slow growing, benign • Cartilaginous (ectopic) • Arise in medullary canal • Children, young adults • Small bones of hands and feet • Multiple • Pathologic fx • Stippled, speckled and ringlikeca++ • Xray, CT, MRI and Nuc med enchondroma
Osteoclastoma • Arise at end of distal femur or prox tibia • Young adult • Epiphyseal closure (20-40 yrs) • Lucent lesion in metaphysis • Extends to subarticular cortex • DOES NOT involve the joint • MRI for extension into soft tissue • Few can be premalignant • “soap bubble” Giant cell tumor
Arise from outer table of skull • Paranasal sinus (frontal/ ethmoid) • Mandible • Incidental due to pain of bone expansion • Well circumscribed, dense, round • < or = to 2 cm in diameter • Osteoid- teenagers • Local pain worse at night (aspirin) • Femur and tibia (<1.5 cm) • Radionuclide bone scan to differentiate from osteomyelitis • Double density • Small round lucent center (nidus) • CT used to enhance nidus with contrast Osteoma/ osteoid Osteomas
Simple bone cyst • unicameral • Fluid filled cyst with wall of fibrous tissue • Proxhumerus or femur @metaphysis • Incidentally or path fx • Expansile lucent lesion • Long axis parallel to long bone • MRI can see if septations are present • Aneurysmal bone cyst • Blood filled arteriovenous communications- caused by trauma • Expansile, eccentric, pronounced ballooning • MRI can demonstrate a fluid level Simple Bone cyst/ Aneurysmal bone cyst
Osteogenic sarcoma • Chondrosarcoma • Ewing’s sarcoma • Multiple myeloma Malignant Bone tumors • soft tissue swelling • Cortical bone erosion • Poor defined margin • Spiculation/ fingerlike • Xray- identify • Radionucleotide/ PET- additional lesions • CT/ MRI detect spread to medullary cavity
Occurs at ends of long bones • Metaphysis • @ knee • Osteoblasts- osteoid/ spicules • Arise in people 10-25 yrs • Small peak incidence in elderly • Paget’s dz • Local pain/ swelling/ fever • Pulmonary edema • No Mets then CT or PET • Mixed destructive sclerotic lesion associated with a soft tissue mass • Periosteal rxn- new bone formation • “Sunburst pattern”- spicules • CT – elevation of periosteum at periphery of a lesion w/ new bone formation • MRI- rule out skip lesions • Treatment- surgical removal, w/ w/o chemo or rad- usually fatal , 30% cured Osteogenic sarcoma
Malignant tumor- • osetochondroma/ enchondroma • Catilagenous • Originate anew or pre-exisiting cartilaginous • Tumor grading- maturity of cells • Long bone • Rib, scapula or vertebrae • ½ as common as osteosarcoma • Develop 35-60 years- grow slowly and mets later • Punctate ca++ • Endosteal scalloping and cortical destruction • Pulmmets- CT • Surgical excision- chemo an rad tx are not suggested- due to poor response • More differentiated > survival Chondrosarcoma
Primary malignant tumor of bone marrow • Children- mid teens, rare over 30 • Local pain, several months • > severity, with tender soft tissue mass • Malise , fever, leukocytosis • Osteomyelitis • Ill defined bone destruction of shaft of long bone • Associated with fusiform layer periostialrxn as “onion skin appearance” • MRI– stage and follow up • Best for soft tissue involvement • Fat sat are best • Rad tx and chemo- chemo make 30%- most die 3-4 years Ewing’s Sarcoma
Disseminated malignancy of plasma cells • Assoc with bone destruction • Bone marrow failure • Hyperca++ • Renal failure • Recurrent infections • Age group is 40-70 • Frequently occurring intramedullary canal of diaphysis • Abnormal spike monoclonal immunoglobulin • Presence of Bence Jones protein in urine • Multiple punched out osteolytic lesions • Lateral views of the skull • Bone destruction is attributed to proliferation of plasma cells • Flat bones- red marrow- vertebrae, skull, ribs and pelvis are primarily affected • Indistinguishable to metastatic cA • Lytic effects are more discrete and uniform in sz • Generalized skeletal deossifications- like postmenoposalosetoperosis • Multiple vertebral compression fxs • Does not cause new bone formation- radio nucleotide scans can be normal • Rad tx and Chemo • Grim prognosis- 3-4 years survival • Pet used for mets and tx effectiveness- active tumor mets Multiple Myeloma
Most common malignant bone tumor • Spread by bloodstream, lymph, or direct extension • Carcinomas- • breast, lung, prostate, kidney and thyroid • Mets to red marrow bones- • Spine, pelvis, ribs, skull, upper hum/ fem • Mets • knee and elbows infrequent- especially bronchogenic ca • Critical in management to know if mets are present • Both at initial staging and follow up care- may exlude pts from radical “curative” tx • offered to those without disseminated dz • Best- Radio nucleotide bone scan- • asymptomatic skeletal mets evaluation- • ½ mineral content of bone must be lost before noticed on general x-ray • Can be confused with multiple myeloma • Due to false (–) bone scan- pts need to be evaluated with xray for symptomatic sites with neoplastic dz unless unequivocal bone scan shows disseminated dz Bone Mets
Broad spectrum • Osteolytic sclerotic or mixed • Mets- distruction w/ out bone proliferation • Develop from tumor embolic deposits • Destroy cortical bone • Irregular/ poorly defined • Most common- osteolyticmets- • Ca of breast , kidney and thyroid • Single large metsforcus • Expansile / trabeculed lesion- “blow out” • Breast- multiple when 1st detected • Spine- involve body and pedicles and posterior arches • Destruction of one or more pedicles are first signs of mets- differentiate from mutlmyloma due to non pedicle involvement • Path collapse in advanced dz • Men- ca of prostate- osteoblasticmets • Women- ca of breast- osteoblasticmets Radiographic appearance of bone mets
Require: • 2 projections at 90 degrees • Demonstrate joint above and below fx • Types • Complete- • discontinuity between 2 or more fragments • Incomplete- • partial discontinuity- portion of cortex intact • Closed- • overlying skin intact • Compound- • overlying skin disrupted/ bone protruding • (open) - immediate • Transverse- • right angle to long axis • Oblique- • 45% to long axis • Spiral- • encircles shaft- longer than oblique- torsional forces • Avulsion- • small fragments from bony prominences- tension on ligaments • Comminuted- • More than 2 fragments • Butterfly • Elongated triangular fragment detached from cortical bone Fractures • Treatment: • Closed reduction= no surgery • Open reduction= surgery- application/ insertion of device to achieve reduction • External fixation- outer device/ splint • Internal fixation- plate, screw, wire, rod
Healing: • Bridge of callus extend across fx line • Malunion- faulty position • Delayed union- ill-defined- longer than average to heal • Nonunion- fx stopped healing • Segmental • Segment of shaft isolated by prox and distal lines of fx • Compression • Compaction of bone trabeculae- vert body/ head of hum/fem • Depressed • Skull of tibial plateau- object of force • Greenstick • Incomplete – opposite cortex intact- children/ infants • Buckle • One cortex and compaction of opposite • Bowing • Deformation from stress, but not enough to fx • Undisplaced • Plane of cleavage in bone with out angle or separation • Displacement/ angulation • Relationship of distal fragments from proximal • Dislocation • Displacement of bone- no longer articulating • Partial= subluxation • stress fractures- repeated stresses to bone, soldiers in basic training- 10-20 after symptoms Types of fractures contd • Pathologic • Occurring in bone weakened by preexisting condition- • METS, multiple myeloma • Children- OI, osteopetrosis, rictets, • Adults- simple bone cyst, osteoporosis, hyperparathyroid • Patients need to be handled with extreme care
Multiple, repeated physically induced injuries to young children • Caused by parents or guardians • Non- accidental trauma • Legal responsibility to report it • Child protective services is involved • When child is being evaluated, diagnosed, treated- the environment must be protective • Shaken baby • Munchausen syndrome by proxy • Sudden infant death • Multiple fx • various stages of healing • Fx at corners of metaphyses • Skull fx Battered-Child syndrome
Colle’s • Transverse, distal radius • Associated avulsion fx ulnar styloid process • Caused by fall on outstretched hand • Navicular • Scaphoid- most common carpal bone • Transverse • Nonunion is serious complication • Avascular necrosis • Boxer’s • Transverse of neck of 5th metacarpal • From a blow struck with the fist • Fractures/ dislocations of spine • Direct trauma, hyperextension-flexion (whiplash), normal stress of abnormal bone (osteoporosis, mets) • Goal of xray- presence of fx and dislocation • C spine injury must have a cross table lateral cleared by a MD • Jefferson- comminuted fx of atlas • Odontoid • Hangman’s- hyperextension- arch of C2- motor vehicle Common fractures/ dislocations
Fibrous outer cartilage (annulus) • Surrounding a central nucleus pulposus (elastic) • Degenerates with age • Herniation can cause severe, acute, chronic, recurring low back pain and leg pain • Most common- L4-L5 and L5- S1 • Causes Sciatica- nerve pain down leg and posterior thigh • Plain xray shows narrowing intervertebral disk spaces, spur formation, • CT, MRI needed to diagnose impression of disk on the spinal cord • Bed rest, muscle relaxant…then surgery Herniation of intervertebral disk
Twisting and curvature • common types • Idiopathic- • young females • Infantile, juvenile and adolescent • Functional- • outside spine, leg length discrepancy • Neuromuscular • Vertebra fail to form completely • Degenerative • Arthritis • Full spine images are obtained- upright • Normal curve= <20 degrees • Curves of 40-50 degrees and >- need extensive tx • Brace and then surgery if curve is 40 degrees or> Scoliosis
Cleft in the pars interarticularis • Usually bilateral • Involve 5th lumbar vertebrae • Predispose the forward displacement of one vertebrae on the other • Chronic back pain • Spondylolysis- defect in the pars • Spondylolisthesis- displacement • Lateral radiograph • Scotty Dog- posterior elements • Pedicle and transverse process- eye and nose • Superior and inferior articular processes- ear and leg • Pars= neck= fx Spondylolysis/ spondylolisthesis