Download
1 / 59
710 likes | 2.42k Views
The Design of Dosage Form. Drugs are administered as a mixture of active ingredient & Excipients. Excipients provide specialized pharmaceutical functions: Solubilize; Suspend; Thicken; preserve; Emulsify; Modify Dissolution; Improve Tablet hardness; Flavors.

E N D
The Design of Dosage Form Drugs are administered as a mixture of active ingredient & Excipients. Excipients provide specialized pharmaceutical functions: Solubilize; Suspend; Thicken; preserve; Emulsify; Modify Dissolution; Improve Tablet hardness; Flavors.
Objectives of Dosage form Design Achieve Predictable Therapeutic Response, Large scale Manufacturing, Reproducible Product Quality.
Required Features to ensure High Product Quality • Chemical & Physical Stability, • Microbiological Stability, • Uniformity of Dose of Drug, • Acceptability to Users, • Appropriate Packaging & Labeling, • Independent patient to patient Variability, • Bioavailability & Bioequivalency.
Factors That Eliminates Bioavailability Variations • Selection of the appropriate chemical form of drug including: • Its Solubility; • Its Particle size; • Its Physical Form; • Manufacturing procedure; • Packaging.
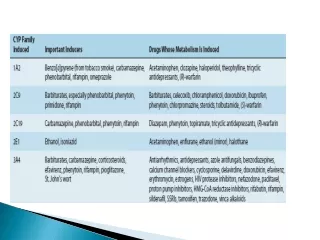
Different Delivery Routs of Drug to Maximize Therapeutic Response (Table 1). • Example 1: Different chemical forms of Prednisolone & formulation additives give a variability of anti-inflammatory preparations such as: • ……………..; • ……………..; • ……………..; • ……………...
Prednisolone • Predinsolone Base & Acetate Salt (…………….. ……………..) is used for: • Tablet & Slow Release I.M. Suspensions; • Predinsolone Phosphate (……………..) is used for: • Soluble tablets, Solutions for eye & ear drops, enema & I.V. injections
Summary • Factors that must be considered for successful Dosage form formulation: • …………….. Factors; • …………….. Factors; • …………….. factors.
Biopharmaceutical Factors • Biopharmaceutics is the study of the relationship between the …………….., …………….. & ……………..sciences applied to drugs, dosage forms & drug action. • Active Ingredient must be in solution form in order to be absorbed. • General Ways for Drug Absorptions: 1. Passive Diffusion, requires: • Gradient of [D]; Appropriate partition coefficient & Degree of ionization. 2. Active transport; 3. Facilitated transport. • Pathways a drug may take following the administration of dosage form by different route (Figure 1). • Variation in time of onset of action for different dosage forms (Table 2).
Routes of Drug Administration Absorption pattern of drugs varies: • Between …………….. substances • Between different ……………...
Oral Route It is the most popular method for drug administration: • ……………..; • ……………..; • ……………..; • Doesn’t need specialized personnel for drug administration; • Drug penetrates the varies GIT epethelia & mucosa; • Gives a systemic effect.
Disadvantages of Oral Route • ……………..; • ……………..; • Destruction of GIT juice dependent drugs; • Interaction of drug with food; • ……………...
GIT pH & Site of Drug absorption • 1 in the ……………..; • 6.8 in the …………….. (Large Absorbing surface); • 7 or 8 in the ……………..; • Weak acid drugs are better absorbed in stomach; • Weak base dugs are preferentially absorbed in the intestine.
Types of Oral Dosage Forms • Tablets, • Capsules, • Powder & Granules, • Suspensions, • Emulsions, • Solutions.
Tablets • Sublingual, • Lozenges, • Chewable, • Effervescent, • Fast release, • Sustained release, • Enteric coated, • Multilayer Tablet.
Capsules • Hard Gelatin Capsules • Soft Elastic Gelatin Capsules
Suspensions & Emulsion 1. Possible administration of large amount of drug, 2. Solve problems of swallowing in pediatric & elderly. Tablets & Capsules 1. ……………..of drugs, 2. ……………..by chewable tablet Advantages of Suspensions & Emulsion in Comparison with Tablets & Capsules
Solutions • Syrups, • Linctuses, • Elixirs.
Rectal Routes • This route of administration is exploited fro systemic & local treatment. • Saving drugs from first – pass metabolism, • Less patient compliance than oral route, • Irregular absorption. Examples: • Solutions, • Suppositories • Emulsions.
Parenteral Route Main Parenteral Routes are: • Subcutaneous (s.c.), • Intramuscular (i.m.), • Intravenous (i.v.), • Intracardiac, • Intrathecal, • Intrasenovial.
Advantages & Disadvantages of Parenteral Route Advantages: • Rabid absorption & Onset of action. • Can be given tounconscious Patients. • Can be given tounable to accept oral medications; • For drugsensitive to GIT juice; • For drugs with poororalabsorption; • Predictable bioavailability.
Continue Disadvantages: • Poor patient compliance; • Need Sterilization; • Need Specialized personnel for drug administration.
Topical Route • Skin is the target organ for both Local & systemic treatment. • Other target organs: eye; nose and ear. Example: • Emulsion (i.e. creams); • Ointments • Gels; • Pastes; • Solutions; • Suspensions.
Advantages: • Good patient compliance; • Ease of administration; • Save drug from GIT juice & First-pass metabolism.
continue Disadvantages: • Poor & Erratic absorption; • Only for small drugs with appropriate partition coefficient; • Skin irritation & sensitization.
Respiratory Route • Lungs are the target organ for both systemic and local treatment. • Drug must be in gaseous, aerosol mist, or ultrafine solid form. • Particles in the range of 0.5-1 µmreachalveolar sacs. • Particles out side this range are either exhaled or deposited upon larger bronchial airways.
Advantages of Respiratory route • Useful for asthmatic patients • Replaces parenteral route in biotechnological drugs proteins (i.e. insulin inhaler).
Drug Factors in Dosage Form Design(Table: 3) To achieve …………….. & …………….. dosage form: • …………….. …………of the drug should be studied; • ……………..of the drug should be studied such as: • Particle ……………..; • Specific ……………..; • …………….. form; • ……………..stability; • ……………..
Particle Size & Surface Area • Particle size reduction results in an ↑ of Asp, which influences: 1. Rate of Drug ……………..; 2. Rate of ……………..; 3. Dosage form …………….. of weight & content; 4. ……………... Poorlysoluble drugs show a dissolutionrate-limiting step (i.e. Greseofulvin, spiranolactone, tolbutamide, ….etc).
Wrong Choice of additives may decrease rate of drug dissolution: • ……………..; • ……………..; • ……………..agents.
Manufacturing process can affect: • Air ……………..on µized powder; • Static charge ……………..; • ……………..& surfaceenergy changes
Solubility • Aqueous Solubility & Therapeutic Efficacy. • Relatively ……………..drugs exhibit ……………..or ……………..absorption. • ……………..& pH: • ……………..& ……………...
Dissolution Noyes-Whitney Equation: dm/dt is the dissolution rate, k is the dissolution rate constant, A is the surface area of dissolving solid, Cs is the [drug] in the dissolution medium at time t(solubility of the drug), C is the initial [drug] in the heart of the solvent.
Partition Coefficient • The ability of a drug to dissolve in a lipid phase when an aqueous phase is also present, often referred to as lipophilicity, can be best characterized by a P defined as the [drug] in the two phases: oil & water
pKa • Henderson-Hasselbalch equation: • A- is the charcged form of the drug (i.e. weak acid) • HA is Uncharged form of the drug • pKa of the drug • pH of the mediam (i.e. stomach, smooth intestin or large intestine)
Crystal Properties: Polymorphism • Practically all drugs are managed in powder form at some stage during their manufacturing into dosage form. • Drug substance can be: • ……………..; • ……………..; • ……………..; • ……………..; • Solvated with other entrapped solvent molecules.
Polymorphism: when drug substance exists in manyforms, with differentmolecularpacking arrangements in the crystal lattice. Generally have different melting points & solubilities, even though they are chemically identical. Almost all long-chain organic compounds exhibit polymorphism.
Theobroma oil (…………….. ) is a polymorphic natural fat. • Theobroma oil can exist in 4 different polymorphic forms of which only one is ……………... • This is important in the preparation of theobroma suppositories. • If the oil is heated to a point where it is completely liquified (about 35 C), the crystals of the stable polymorph are destroyed & the mass does not crystallize until it is cooled to 15 C. • The crystals that form are unstable & the suppositories melt at 24 C. • Theobroma suppositories must be prepared below 35 C.
Different polymorphs exhibit different ……………...: one polymorph may be more active than another (e.g.,……………..). Polymorphism can also be a factor in ……………..technology. Cortisone acetate has been found to exist in at least 5 different forms, 4 of which are ……………..in water & change to the ……………..form.
Abbott Laboratories had to withdraw their HIV………………….. drug, ………………….., from the market due to the fact that an unwanted ………………….. of the drug had been produced during …………………... Instead of Capsules consisting entirely of the known ………………….. of the drug, a new polymorph, named Form II………………….., was ………………….. in the capsules.
This form had a different ………………….. rate so the ………………….. of the final capsule was affected. Production of the capsules had to stop immediately until the problems with the ………………….. process could be rectified. Patients using the drug had to rel ………………….. on a ………………….. form until manufacturing could be resumed. Abbott could not risk supplying their patients with a polymorph that ………………….. in bioavailability.
Insulin Polymorphism Insulin + Zn (in presence of Acetate buffer) produces an extremely …………………... Depending on the environmental pH the resulted complex can be: • ………………….. precipitate [contains particles with no uniform shape & < 2µm, which can be absorbed after s.c. or i.m. injection with short t1/2]]
2. Crystalline product [contains ………………….. crystals consisting of 10-40 µm size, which can be absorbed more slowly & has a longer t1/2]; 3. Physical mixtures of these two products gives insulin preparation with intermediate t1/2
Polymorphic Transition • Polymorphic transition can occur: • During …………………..; • During …………………..; • During …………………..; • During …………………...
Stability • Chemical, Physical & Microbiological stability of the formulation must be ensured during the usable life of the drug. • Chemical changes involve the additives also. • Packaging of the dosage form is an important contributing factor to product stability.
Classification of drugs according to their sensitivity to breakdown • Stable under …………………..(e.g. kaolin) • Stable if handled …………………..(e.g. aspirin) • Moderately stable …………………..(e.g. vitamins) • Very unstable or …………………..(e.g. -lactams in solution)
Solid-State degradation Mechanisms of solid-state degradations are complex & oftendifficult to analyses. When drug is water sensitive precautions such as: • Minimum exposure to …………………..; • Low moisture content …………………..; • Moisture resistant …………………... For ………………….. drugs antioxidants should be included in the formulation. For light-sensitive drugs, ………………….. should be used.