Download
1 / 40
590 likes | 1.31k Views
Anticoagulants and Antiplatelets. Presenter: Dr. Ashish Chakravarty MD student Moderator: Dr. Kavita Sharma Professor Dept. of Anesthesiology and Intensive Care, MAMC, New Delhi . www.anaesthesia.co.in anaesthesia.co.in@gmail.com. What u’ll be served for lunch today…!!. Appetizers:

E N D
Anticoagulants and Antiplatelets Presenter: Dr. Ashish Chakravarty MD student Moderator: Dr. Kavita Sharma Professor Dept. of Anesthesiology and Intensive Care, MAMC, New Delhi www.anaesthesia.co.in anaesthesia.co.in@gmail.com
What u’ll be served for lunch today…!! • Appetizers: • Basic pathophysiology of hemostasis • Basic pharmacology of antithrombotics,anticoagulants, and thrombolytics • Whole course: • An intensivist’s perspective regarding usage of these drugs • An anesthesiologist’s perspective for an elective case • Dessert: • An anesthesiologist’s perspective for an emegency case • Some food for thought !!
Terminologies • Antithrombotics = Drugs which interfere with platelet functions • Anticoagulants = Drugs used to reduce the coagulability of blood • Thrombolytics (Fibrinolytics) = Drugs used to lyse thrombin clot (mainly therapeutic)
Functions of Platelet • Plug formation by passive “agglutination” and active “aggregation” – later reinforced by fibrin • Exposure of PF3which is clotting factor III • Mechanical clot retraction involving platelet actin and myosin - strengthens clot • Active biochemicals from α granules, dense granules and cytoplasm
…contd • α granules • vWF • Dense granules • ADP* • Ca2+ • Serotonin • Adrenaline • Cytoplasm • TxA2* • Fibrinogen • TFPI (tissue factor pathway inhibitor)** • Receptors associated with platelets • GP Ib : links vWF • GP IIb/IIIa : links fibrinogen* • Granules : • Release their contents • Expose their inner phospholipid surface • which is PF3
Antiplatelet activity in the body • Invivo blockers of platelet aggregation • PGI2* through cAMP* pathway • NO through cGMP pathway Produced in vascular endothelium
Antiplatelet pharmaceuticals • NSAIDS – inhibit cyclooxygenase and decrease TxA2 synthesis (irreversibly with Aspirin) • Ticlopidine and Clopidogrel – ADP induced platelet aggregation & platelet-fibrinogen interaction irreversibly blocked • Cilostazol: PDIII inhibitor – increases cytoplasmic cAMP • GP IIb/IIIa blockers : Abciximab,Eptifibatide, Tirofiban • Dextran : interferes with platelet aggregation
Antiplatelet phamaceuticals…contd • Dipyridamole # Increases PGI2 release from the endothelium # Inhibits platelet phosphodiesterase - builds up platelet cAMP and decreases cytoplasmic Ca2+ # Inhibits RBC uptake of adenosine* which is an inhibitor of platelet reactivity # Inhibits the formation of TxA2 by blocking Tx synthetase
The Coagulation Cascade XIIIntrinsicTFExtrinsic* HMWH PK XI VIIa* VII XIIa Ca2+ IX HMWK Ca2+ XIa VIIa/TF* IXa Ca2+ Ca2+ PF3 VIII VIIIa* X Xa* Ca2+ PF3 V Va* IIa II Fibrinogen Fibrin monomer Fibrin polymer XIII XIIIa Cross-linked fibrin polymer
Coagulation Cascade…contd.. • Three steps: • Initiation Phase: • Starts with VIIa/TF • Ends with formation of IIa • Amplification Phase • Activation of V, VIII, XIII, XI and Fibrinogen by IIa, if the IIa is not neutralised by ATIII or Thrombomodulin • Propagation Phase • Refers to the phase during which activated factors Va, VIIIa, and IXa attach to the platelets and the platelets release PF3
Coagulation Cascade…contd.. • All clotting factors are serine proteases except V and VIII which are coenzymes, and labile factors • The serine proteases ( but not co-enzymes) are activated by Ca2+ • TF and PF3 activate the clotting factors by attaching to Ca2+ which in turn attach to the clotting factors (serine proteases) by 2 –ve charge on their carboxyl group. • Vit K carboxylates factors II, VII, IX, X and Protein C & S thereby providing the needed 2-ve charge for binding to Ca2+
In-vivo Antithrombotic Mechanisms • Antithrombin III • Inhibits IIa, IXa, Xa, XIa, XIIa, XIIIa and Plasmin by binding to their active site • When heparin bind to AT III the active sites of the clotting factors are further compromised • Acquired AT III deficiency: DIC, OCP, sepsis, c/c heparin Rx • Protein C & S • IIa + Protein C Protein Ca Va & VIIIa inactivation • Protein S is a co-factor for activated Protein C (Protein Ca) • Tissue factor pathway inhibitor (TFPI) • Inhibits VIIa/TF complex and Xa • Circulates in Plasma or contained in Platelets or on Endothelium • Heparin may release it from the surface of endothelial cells • Fibrinolysis
The Fibrinolytic System Plasminogen tPA Urokinase (endothelium) PAI-1 PAI-2 Thrombin (IIa) Plasmin (α2 antiplasmin) PI Cross-linked fibrin polymer Fibrinogen fibrin Polymer FDP D-Dimer
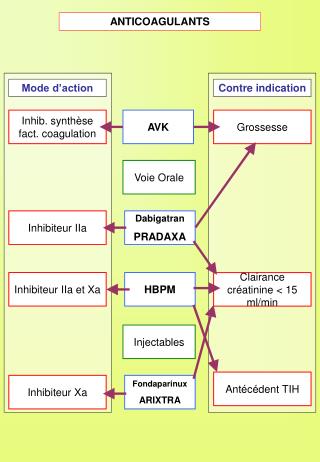
Anticoagulant pharmaceuticals • Standard Heparin (Unfractionated Heparin) (mol.wt 5000- 30,000 Da; av.15,000 Da) • Derived from porcine intestinal mucosa or beef lung, prepared as Na+ or Ca2+salts • AT III inhibits IIa, IXa, Xa, XIa, XIIa, XIIIa and Plasmin by binding to their active site. When heparin binds to AT III the active sites of the clotting factors are further compromised • Routes: IV, SC, Intra nasal. Never IM or Oral* • Peak plasma levels after SC inj. 2-4 hrs. • Strongly anionic, hence rapidly bound to proteins….t1/2 90 min
Heparin…contd • Complications • Hemorrhage…esp. intracranial, intraspinal, intraocular • Heparin resistance…seen in a/c thrombotic processes with consumption of AT III. Rx FFP !! • Maternal osteoporosis on c/c use • HIT Syndrome: spectrum • Thrombocytopenia without thrombosis • Hypotension & Transient reversible platelet aggregation • Irreversible platelet aggregation: White clot syndrome • Heparin antibodies
LMWH • M.Wt 2000-8000 Da ( avg 4500 Da )- prepared from SH by fractionation, enzymatic degradation or chem modifn • Commercial preprn : Enoxaparin, Dalteparin, Ardeparin, Tinzaparin, Fondaparinux • Routes : SC (OD) • High anti-Xa and low anti-IIa activity↔ greater antithrombotic and lower anticoag activity • Low anti-IIa activity, hence, aPTT, TT, ACT not ideal for monitoring. Anti-Xa assay ideal • Less complicated, dose independent clearance and more predictable anticoagulant response than SH. Hence lab monitoring not required • Fondaparinux: synthetic, specific inhibitor of Xa, used for Px in THR & TKR. Long elimination t 1/2 (20 hrs). Renal clearance
Anticoagulation with SH & LMWH Indication SH Target PTT LMWH venous thrombosis Rx 5000 U I.V bolus; 2-2.5 100 U/kg SC 1000 U/hr BD Px 5000 U SC BD-TDS < 1.5 “” AMI With TLT 5000 U I.V bolus; 1.5-2.5 100 U/kg SC 1000 U/hr BD With mural 8000 U SC TDS + 1.5-2 “” thrombus Warfarin Unstable Angina 5000 U I.V bolus; 1.5-2.5 100 U/kg SC 1000 U/hr BD Prophylaxis General surgery 5000 U SC BD < 1.5 100 U/kg SC before and BD Ortho surgery 10000 U SC BD 1.5 “” CHF/ MI 10000 U SC BD 1.5 100 U/kg SC BD
Targeting PTT • Normal PTT (27- 35 s) – 5000 U i.v bolus; 1300 U / hr infusion. Monitor PTT • Recheck PTT: 35- 50 s – rebolus 5000 U; increase infusion by 100 U / hr • Recheck PTT: 50- 60 s – increase infusion by 100 U / hr • Recheck PTT: 60- 85 s – NO CHANGE • Recheck PTT: 85- 100 s – decrease infusion by 100 U / hr • Recheck PTT: 100- 120 s – stop infusion for 30 min, and decrease infusion by 100 U / hr at restart • Recheck PTT: > 120 s – stop infusion for 1 hr, and decrease infusion by 200 U / hr at restart
Heparin-free CPB • WHY? • Hemorrhage, HIT syndrome, Heparin allergy • HOW? • Heparin of different biological source • Chlorocresol-free heparin • Methylprednisolone Px, H1blockers • Heparin with ‘iloprost’ (PGI2analog) • Ancrod: protease: removes fibrinopeptide A from fibrinogen: prevents fibrin cross-linkage. Monitor with fibrinogen levels. Reverse with cryoppt. • Danaparoid: LMW heparinoid anti Xa:IIa ratio = 22:1. Minimal effect on platelets. Monitor anti Xa assay. Renal excretion. Difficult to eliminate as t ½ > 24hr. Reverse with plasmapheresis • Recombinant hirudin: highly specific for thrombin. Monitor aPTT. Renal excretion. t ½ 30-60 min. no antagonists • Argatroban: synthetic direct thrombin inhibitor. Not available yet
Anticoagulation with SH & LMWH …contd • Other uses: • To prevent catheter thrombosis: 2-5 U/ml • If sample collected from indwelling catheter, blood to be discarded prior to collection of the sample = 3 times the volume of catheter. • For ABG: 1000 U/ml. Don’t exceed 1/10th the volume of blood, since heparin is itself acidic…. may alter results • Temporary vascular occlusion: 100 U/kg • For CPB & ECMO: 300 U/kg. Monitor ACT. Reverse with Protamine 1mg / 100 U Heparin
Coumarin derivatives • Dicumarol and Warfarin • Indirect anticoagulants- interfere with hepatic synthesis of Vit K- dependent clotting factors • Used for Px and Rx in thrombophlebitis, AF, PTE, AMI, mechanical prosthetic valves and valvular heart disease • A typical regimen: warfarin started at 5mg/day x 7days, then maintenance dose 2.5 to 7.5 mg OD depending upon required INR • Monitored using Prothrombin time & INR
INR • INR= (PTTest/ PTControl)ISI • ISI (International Sensitivity Index) of the thromboplastin reagent used in a specific coagulometer is assigned by the manufacturer. • INR should not vary by reagent or equipment • Only 30% of the normal concentrations of clotting factors is adequate to maintain a normal INR • Hypofibrinogenemia will influence INR when its concentration goes below 80 mg% • Therapeutic range of INR varies with different clinical condition. Thus hemorrhage may occur even within the therapeutic range.
INR…contd.. • INR target ranges for oral anticoagulation: Condition INR DurationVenous thrombosis Rx 2-3 3-6 month Px 1.5 c/c AF 1.5-2 c/c MI 2-3 2-3 month Heart valves Tissue valves 2-2.5 c/c Mechanical 3-4 c/c CMP 2-3 C/C
INCREASE PT Reduced clearance Disulfiram Metronidazole cotrimoxazole Reduced albumin binding Phenylbutazone Additive hemostatic effect Aspirin, Heparin Liver disease, Vit. K deficiency Incresed turnover of Vit.K Clofibrate, Hypermetabolic state DECREASE PT Accelerated clearance Barbiturates Rifampin Reduced absorption Cholestyramin Coumarin resistance Factors affecting coumarin potency
Fibrinolytics • Plasminogen activators • Preparations: • Anistreplase (t ½ 100 minutes) • Streptokinase (t ½ 83 minutes) • Urokinase (t ½ 20 minutes) • Reteplase (t ½ 15 minutes) • Alteplase (t ½ 3 minutes) • Streptokinase: • bacterial enzyme • indirect activator of plasminogen: SK first forms a complex with Plasminogen. It is this complex which activates subsequent plasminogen. • Dose in AMI: 1.5 million units I.V over 1 hour • Urokinase: • product of renal tubular cell • direct activator of plasminogen.
Fibrinolytics…contd.. • Major problem: hemorrhage • Causes: • NOT related to residual activity • Defective fibrin polymerisation due to FDPs: can be a problem upto 24 hrs despite t1/2 of 3 hrs • Platelet aggregation inhibition by FDPs • Decreased concentration of factors I,V & VIII • Rx of hemorrhage due to fibrinolytics: • Discontinue administration • Antagonise residual effect: Aprotinin or EACA • After residual effect wanes: FFP / Cryoppt
Fibrinolytics…contd.. • Some basic facts to be remembered: • Heparin should be added in the post-thrombolytic pd. till hospitalised followed by warfarin therapy till 3 months, as Plasminogen is most effective if it lies within the fibrin matrix during clot formation. Clots formed during the period of thrombolysis are resistant to subsequent thrombolysis. • Reperfusion arrhythmia: so must repeat an ECG post-thrombolysis • Avoid coughing, straining, HTN post-thrombolysis • No IM inj. • Sampling through indwelling catheters • Lower limb BP cuffs: risk of embolisation of dissolving clots • Local infusions of thrombolytics may have major systemic effects: Do Not Underestimate !
Fibrinolytics…contd.. • Contraindications: • Absolute • Cerebrovascular hmg at any time • Non hmgic stroke or other CVA within past year • SBP >180mmHg; DBP >110 mmHg • Suspicion of Aortic dissection • Active internal bleeding (excluding menses) • Relative • INR ≥ 2 on current anticoagulant • Recent (< 2 wk.) history of surgery or invasive procedure • Prolonged ( > 10 min )CPCR • Known bleeding diathesis • Pregnancy • Hmgic ophthalmic condition (eg. hmgic diabetic retinopathy) • Active peptic ulcer • history of severe HTN, now adequately controlled • history of having received SK within 5 days to 2 years
Neuraxial block along with anticoagulants: Recommendations • Antiplateles • NSAIDs alone and NAB are compatible • The effect of ticlopidin and clopidogrel should be allowed to dissipate (7 days) before NAB • GPIIb/IIIa inhibitors: NAB 8 hrs after tirofiban and eptifibatide, and 48 hrs after abciximab • Concurrent use of SH, LMWH, or anticoagulants increase the risk of bleeding (holds true for all subsequent anticoagulants) • Fibrinolytics • NAB not recommended upto 10 days • If NAB is undertaken, monitor neurologically atleast q2h • Confirm adequate fibrinogen and low FDP levels before removing the catheters
…contd.. • Oral anticoagulants • Stop anticoagulants and allow normalization of INR prior to performance of NAB • Preop warfarin: if initial dose >24 hrs earlier or a second dose was given, check INR before NAB • Warfarin @ 5mg/day for >36 hrs and receiving epidural analgesia should have INR checked daily and before catheter removal • If epidural catheter present, withold / reduce warfarin if INR > 3 • Remove catheter if INR < 1.5 • If INR > 1.5 and catheter removed, monitor neurologically for at least 24 hrs.
…Contd.. • Standard heparin • Minidose, SC • No CI to performance of NAB • Consider delaying initiation of heparin till after institution of the NAB • After 4 days of SH confirm whether HIT has occurred • I.V Heparin for intraop anticoagulation • A gap of 4-6 hrs required between heparin and NAB • Consider minimal concentrations of local anesthetics to permit early detection of neurological changes • Delay initiating heparin till 1 hr after needle placement for NAB • Remove epidural cath 1 hr before any subsequent i.v dose of heparin (assuming 12 hrly dosing ) or 4 hr after the last dose of heparin • Difficult needle placement / bloody tap not an indication for cancellation, but frequent postop monitoring of neurological status mandatory
…contd.. • LMWH • A gap of 24 hrs required between Fondaparinux administration and NAB. For catheter removal same interval recommended • A gap of 12 hrs required between LMWH and performance of NAB. In renal failure the interval should be longer (16-18 hrs) • Remove epidural cath 24 hr after last dose of LMWH and do not administer subsequent dose for next 2 hr • Difficult needle placement / bloody tap not an indication for cancellation, but important to delay subsequent dose of LMWH for 24 hrs • Consider minimal concentrations of local anesthetics to permit early detection of neurological changes • Consider single dose SAB • Prompt recognition of epidural hematoma is confirmed by CT or MRI followed by emergency decompressive laminectomy within 8 hrs
Anticoagulants and periop considerations • Advantages of stopping an anticoagulant should outweigh the risks • Postop bleeding due to warfarin administration is rarely fatal or associated with major morbidity whereas the consequences of venous or arterial embolism may be fatal • Anticoagulation decreases the risk of VTE by 80%, the risk of arterial TE in patients with mechanical heart valves by 75%, and risk of ATE in patients with nonvalvular AF by 66% • Rebound hypercoagulation state may develop by discontinuing warfarin, super-added by the prothrombotic effect of surgery . • Surgery increases risk of VTE but not ATE in patients with AF or mechanical heart valves
Patients on warfarin periop • In cases where change over to alternative anticoagulant not done before sx: • INR 2-3: 4 scheduled doses of warfarin withheld to allow INR to fall to ≤ 1.5 before sx • INR measured day before sx to see response • If INR ≥ 1.8 at this time, inj. Vit. K SC (not IM) • If INR ≤ 1.5 perform surgery • After surgery: • Warfarin takes 3-4 days to reach INR to 2. So Rx started soon after surgery • With the above regimen patients can have subtherapeutic levels for 2 days before and after surgery. Yet these levels can still provide partial protection against thromboembolism
Patient on warfarin for VTE • During first 30 days: • Elective surgery should be avoided • If not possible, substitute with I.V Heparin before and after surgery while INR <2 • If PTT within Rxic range, stop heparin 4-6 hrs prior to surgery • Restart Heparin 4-6 hrs after surgery, but do not infuse @ greater than the maintenance rate for about 12 hrs. Should be delayed even longer if evidence of surgical bleed • PTT rechecked 12 hrs after restarting heparin • After 30 days: • Discontinue warfarin 4 days prior • Need not start I.V Heparin preop • I.V Heparin must be started postop and continued till warfarin takes effect and INR ≥ 2.0 • Mechanical Px should be combined
Recommendations for periop anticoagulation in patients on warfarin Indications Before sx After sx Acute VTE / ATE (first 30 days) I.V Heparin I.V Heparin VTE after 30 daysno changeI.V Heparin Recurrent VTE no change SC Heparin Mech. Heart valve no change SC Heparin Non-valvular AF no change SC Heparin
Patients on other anticoagulants • Clopidogrel: should be stopped 7 days before surgery. Aspirin can be substituted safely • GPIIb/IIIa inhibitors: contraindicated upto 6 wks after major trauma or surgery • Fondaparinux: administered 6 hrs after surgery
What if…? • Emergency surgery ? • Aspirin- not much bleeding • Clopidogrel- platelet concentrates. • UFH poses not much problem- can be stopped 4 hrs prior. May be reversed with protamine. FFP may be administered • LMWH: needs to be stopped 12 hrs earlier…what if accompanied by renal failure? • Warfarin: now u have a problem. Vit K starts to act within 8-12 hrs…what route will u give?Menadione sodium diphosphate i.v. Try FFP.
What if…? • Dire emergency? (“half-hour ot time”) • Platelet concentrates, protamine, FFP • A lot of prayer !!
THANKYOU www.anaesthesia.co.in anaesthesia.co.in@gmail.com