Download
1 / 25
250 likes | 629 Views
Feeding the preterm IUGR infant. Prof Sanjay Patole, MD, DCH, FRACP, MSc, DrPH Centre for Neonatal Research and Education KEM Hospital for Women, University of Western Australia Perth. Feeding preterm IUGR infants.

E N D
Feeding the preterm IUGR infant Prof Sanjay Patole, MD, DCH, FRACP, MSc, DrPH Centre for Neonatal Research and Education KEM Hospital for Women, University of Western Australia Perth
Feeding preterm IUGR infants • Experimental studies show that hypoxia reduces intestinal blood flow and oxygen delivery through adrenergic vasoconstriction. Nowicki et al 1988 • ↑ Oxygen extraction can compensate for a 30% reduction in gut blood flow, but enteral feeding reduces the ability of oxygen extraction to compensate for the effects of hypoxia. Bulkley et al 1985, Szabo et al 1987 • Metabolic demands of enteral feeds increase O2 consumption by the intestine. Nowicki et al 1983
Feeding preterm IUGR infants SMA and Coeliac axis flow is significantly reduced on D1 and the recovery in the baseline flow is slow during the 1st week of life in IUGR infants Despite the recovery in baseline SMA and Coeliac axis flow, the dynamic response to 1st feed is still impaired in IUGR infants Gamsu 1997, Maruyama 2001, Murdoch 2003
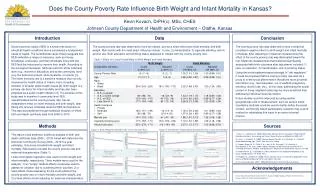
Feeding preterm IUGR infants: Perth data 38/220 (17.3%) neonates < 28 weeks during 2 year period had IUGR. Mean (IQR) age at start of feeds: 7 (5-10) vs. 5 (4-8) days, p = 0.005 Mean (IQR) age at 1 ml/2hourly feeds: 12 (8-15) vs. 9 (7-13) days, p = 0.034 Shah et al JMFN Med 2014
Feeding preterm IUGR infants Median (IQR) postnatal age at FEF (150 ml/kg/day): 32 (21-40) vs. 24 (17-31) days, p = 0.009 Postnatal growth restriction: 73% vs. 45%, p = 0.003 Definite NEC: 18/220 (8.1%) Conclusion: Optimising enteral nutrition in extremely preterm IUGR neonates is a difficult proposition Shah et al JMFN Med 2014
Preterm IUGR infants and abnormal Dopplers Independent case series (N=14) All NEC: AREDF: 85/659 vs Control: 66/1178 OR: 2.13 (95% CI: 1.49 to 3.03) Confirmed NEC (6 studies): OR: 6.9 (95% CI: 2.3 to 20) Dorling et al. ADC2005
Santulli theory for pathogenesis of NEC: Triad of ischaemia, bacteria, and substrate Santulli et al. Pediatrics 1975 Prolonging small feeding volumes early in life decreases the incidence of NEC in VLBW infants. Berseth et al. Pediatrics 2003
Early feeding advancement in VLBW infants with IUGR and ↑ UA resistance 124 inborn VLBW infants enrolled in a prospective trial evaluating early enteral nutrition after a standardized feeding protocol (daily feed increment: 16 ml/kg) Feeding tolerance assessed by age at FEF (150 ml/kg/day) Mihatsch et al. JPGN2002
Results FEF achieved at 15 days (12-21 days) of age for all infants. IUGR [FEF: 14 (12-21) days], ↑ UA resistance [FEF: 14 (11-16) days], and brain sparing [FEF: 15 (14-20) days] were not associated with early feed intolerance. Conclusion: VLBW infants with IUGR, ↑ UA resistance, and brain sparing tolerated enteral feeds as well as AGA VLBW infants.
Early versus delayed MEF and risk for NEC in preterm IUGR infants with abnormal Dopplers. Aim: Assess the effect of early (≤5 days) vs. delayed (≥6 days) MEF on the incidence of NEC and feed intolerance in preterm IUGR infants with abnormal Dopplers. Design: Randomized, non-blinded pilot trial: “Early” vs. “Delayed” MEF in addition to PN within 48 hours Karagianni et al. 2010 May
Results • 81/84 enrolled infants completed the trial • 40 Early: 2 (1-5) vs. 41 Delayed MEF: 7 (6-14) days • No significant difference in NEC (p=0.353) and feeding intolerance (p=0.533)
Results Birth weight was an independent risk factor for NEC in both groups. Early MEF may not have a significant effect on NEC or feed intolerance in preterm IUGR infants with altered Dopplers.
Predictors of NEC in preterm IUGR neonates • Even when Doppler variables are taken into consideration, birthweight remains the predominant risk factor for NEC. Manogura AC et al. Am J Obstet Gynecol. 2008
Early vs. delayed enteral feeding for preterm growth-restricted infants: a randomized trial Leaf et al. Pediatrics 2012 May
Background Preterm IUGR infants are at increased risk of NEC and delayed initiation of feeds No evidence that this delay is beneficial and might further compromise nutrition and growth
Methods Infants with gestation <35 weeks, BW <10th centile and abnormal UA Doppler waveforms randomly allocated to: Start feeds "Early" (D2) or "Late" (D6) after birth Feeds ↑ gradually by a feeding protocol, equal rate of increase for both groups Primary outcomes: Time to FEF sustained for 72 hrs and NEC
Sample size estimation Unpublished data from a UK regional database of VLBW revealed an SD of 9 days in the time to reach FEF 380 infants needed to show a 3 day difference in time to FEF with 90% power NEC:15%, so recruiting 400 infants would be sufficient to show a 50% change in the incidence of NEC with 60% power
Results 404 infants from 54 hospitals in UK and Ireland (202/group) Median gestation: 31 weeks FEF (Median): Early 18 vs. Late 21 days (HR: 1.36; 95% CI: 1.11-1.67) All Stage NEC: Early 18% vs. Late 15% (RR: 1.2; 95% CI: 0.77-1.87) Stage II/III NEC: 8% in both groups Early feeds: Shorter duration of TPN and high-dependency care, ↓ cholestasis, and ↑ SD score for weight at discharge
Conclusion Early introduction of feeds in preterm IUGR infants resulted in earlier achievement of FEF without increasing the risk of NEC
Applicability of ADEPT trial results Gestation <29 weeks: 44 vs. 42 infants Birth weight <1000 grams: 86 vs. 105 infants Birth weight < 750 grams: 33 vs. 41 infants Not powered adequately for detecting a minimum significant change in incidence of NEC, the real concern Enrolment from 64 centres No real justification for late starting of feeds (after 6 days)
Post-hoc analysis: ADEPT subgroup IUGR neonates <29 weeks failed to tolerate even the careful feeding and reached FF significantly later than predicted Median (IQR) age at FEF in <29 vs ≥29 weeks: 28 (22-40) vs. 19 (17-23) days, HR 0.35 (95% CI: 0.3 to 0.5) Incidence of NEC significantly higher in <29 vs ≥29 weeks: 32/83 (39%) vs. 32/312 (10%), RR: 3.7, (95% CI 2.4 to 5.7) Kempley et al. ADC 2013 Aug
Other risk factors • PDA • Ibuprofen • Phototherapy • CPAP • Proinflammatory cytokines (PIH) • Oxidative stress • Sepsis (neutropenia) • Polycythemia
Minimising the risk of NEC in IUGR neonates Early trophic enteral feeds Early preferential use of mother’s milk PDHM if mother’s milk is unavailable/Avoid formula Feeding protocol (Conservative vs. Aggressive) Ideal vs realistic nutritional goals Prevention and treatment of sepsis Probiotic supplementation
NEC: Unusual presentation in preterm IUGR No significant abdominal distension, minimal bile stained gastric residuals, no/no significant pneumatosis but Significant widespread necrosis of the gut on autopsy
Feeding preterm IUGR infants <28 weeks Start colostrum as soon as available (Day 0) Early trophic feeds: <10 ml/kg/day, Duration: 5 days Nutritional feeds: Start at 15 ml/kg/day and↑ by 15 ml/kg/day Consider continuous feeds for persistent feed intolerance Reach 60 ml/kg/day to promote gut development and function Worsening volume and colour of gastric residuals: Take a break!! Clinical examination, and awareness of coexisting risk factors for NEC are important Probiotic supplementation (Will they work?)