Download
1 / 22
240 likes | 1.29k Views
Kidney- Tubulo -interstitial disorders. Acute Kidney Injury (Acute Tubular Necrosis). Most common cause of Acute Renal Failure (ARF) Acute reduction in renal function with tubular injury Two types: Ischemic Toxic

E N D
Acute Kidney Injury(Acute Tubular Necrosis) • Most common cause of Acute Renal Failure (ARF) • Acute reduction in renal function with tubular injury • Two types: • Ischemic • Toxic • Rapid reduction of renal function & urine flow-falls within 24hrs to < 400mL / day. What causes AKI? 1. Ischemia: • Malignant Hypertension • DIC • Microscopic polyangitis • Hemolytic Uremic Syndrome (HUS). • Thrombotic thrombocytopenic purpura. • Direct Toxic Injury- Drugs like Gentamycin. 3. Acute TubulointerstitialNephritis - hypersensitivity reaction to drugs. 4. Urinary obstruction-tumors, BPH, blood clots.(Post renal causes)
ATN or AKI -2 Types Ischemic: • Discontinuous ,focal involvement at multiple points. • Tubulorrhexis. • Tubular lumen- casts-both hyaline & pigmented granular casts - Tamm-Horsfall protein. • Regeneration –is complete. Toxic: Mercuric chloride,CCl4 • Continuous – mainly PCT. • No B.M rupture.
Clinical course of AKI. 1. Initiation phase- lasts 36 hrs.-dominated by the cause ie, the inciting medical, surgical or obstetric event. Slight ↓ in renal output with ↑ BUN 2. Maintenance phase: sustained ↓ in renal output -40-400mL/day (oliguria), salt & water overload, ↑ BUN concentrations, hyperkalemia, metabolic acidosis, uremia. *Balance of water & electrolytes-crucial in this stage; Dialysis. 3.Recovery Phase: steady ↑ in urine volume upto 3L/day . Loss of water & electrolytes due to tubular damage. Hypokalemia. Eventually tubular concentrating ability returns. Takes time; but recovery is complete- depending on the initiating cause. In shock related to sepsis, burns etc-50% mortality.
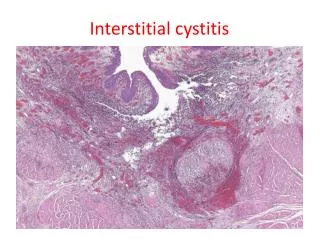
Tubulointerstitial nephritis. • Acute & Chronic Pyelonephritis. 2. UTI-Urinary tract infection • Vesicoureteric reflux • Intrarenal reflux. • In the absence of VUR, the infection remains in the bladder-cystitis & urethritis.
Both poles of kidney UTI-routes of infection Voiding Cystourethrogram-Vesico-ureteric reflux
Acute Pyelonephritis *Hallmarks: • Patchy interstitial suppurative inflammation. • Neutrophil aggregates in the tubular lumen • Tubular necrosis. *Secondary to bacterial and viral*(polyoma) infections Complications: • Papillary necrosis • Pyonephrosis • Perinephric abscess
Grey white areas on cortical surface-abscesses Acute inflammatory cells within tubules & interstitium Polyoma virus-intranuclear inclusions.
Papillary necrosis. Tips of the pyramids show necrosis. Grey white to yellow necrosis-arrows. Papillary necrosis is also seen in: Diabetes Analgesic nephropathy Sickle cell disease Urinary tract obstruction
Chronic Pyelonephritis • A rare variant is Xanthogranulomatouspyelonephritis characterized by the presence of: - Foamy macrophages - Plasma cells and lymphocytes - Giant cells - Proteus infection is common • Chronic inflammation of tubules, interstitium, calyces and pelvis with extensive scarring • Condition can be bilateral • Asymmetric irregularly scarred kidneys • Microscopically: • Atrophic glomeruli • Periglomerular fibrosis • Atrophic tubules • Tubular lumen containing secretions simulating thyroid gland and hence the name “thyroidization’ of kidney
Hallmark of Chronic Pyelonephritis: Coarse, discrete corticomedullary scars overlying dilated, blunted calyces; flattening of the papillae. Irregularly, asymmetrically scarred kidneys
Chronic Pyelonephritis Chronic inflammatory cells in the interstitium; Tubular atrophy or dilatation; Fibrosis. Dilated tubules filled with colloid casts- “thyroidization”
Drugs & Toxins • Drugs and toxins can produce renal injury in 3 ways: • Trigger interstitial immunologic reaction eg.acute hypersensitivity reaction by methicillin. • ARF • Subtle, cumulative effect—over yrs—CRF. Drugs: • Sulfonamides • Methicillin, ampicillin, • Rifampicin, • Thiazide diuretics, • NSAIDS • Allopurinol, • Cimetidine Clin:Fever, skin rash, eosinophilia,renal abnormalities -about15 days after taking the drug.
Acute drug-induced interstitial Nephritis. • Interstitium-edema • Infiltration by lymphocytes, macrophages. • eosinophils & neutrophils may be seen in clusters. • Plasma cells, basophils-small number. • Glomeruli-normal;except sometimes in NSAIDS-minimal change & N.S develop. • Important to recognise, as withdrawal of the drug –causes reversal – but it takes time.
Analgesic Nephropathy.* Phenacetin • Was one of the leading causes of end-stage renal disease in Australia & other countries until public health measures reduced the sale of over-the-counter medications containing these mixtures. • Due to excessive intake of analgesic mixtures containing Phenacetin, aspirin, caffeine & codeine. • More common in women suffering from psychoneurotic illness • Causes papillary necrosis first and tubulointerstitial nephritis next. Papillae may be sloughed off in to the urine. • Complications include the development of transitional cell carcinoma of the renal pelvis in a small% of patients Papillary necrosis.
Nephropathy associated with NSAIDS. Aristolochic Nephropathy. • Uncommon, but should be kept in mind. • The selective COX-2 inhibitors ,while sparing the GIT, may damage the kidneys. • ARF • Acute hypersensitivity interstitial nephritis • Acute interstitial nephritis & MCD • Membranous Nephropathy with the N.S • Aristolochic acid is found in certain herbal medications. • The drug forms co-valent adducts with DNA & causes a distinctive picture of renal failure & interstitial fibrosis; associated with a relative paucity of infiltrating leukocytes. • ↑ incidence of carcinoma in the kidney & urinary tract. • Also the cause of Balkan nephropathy.
Urate Nephropathy. • Acute uric acid nephropathyshows crystals in the tubules (C.Ds)– obstruction and renal failure; seen in patients who are on chemotherapy for leukemias;lymphomas. • Chronic urate(Gouty) nephropathy (Gout-1243-6)- with hyperuricemia – deposition of monosodium uratecrystals in the acidic distal tubules &CDs. • Birefringent needle-likecrystals in tubular lumen or interstitium. • Nephrolithiasis – presence of uric acid stones – found in gout and secondary hyperuricemia. Giant cell reaction & fibrosis around the crystals.
Light-chain cast Nephropathy/Myeloma Kidney • BenceJones proteinuria & cast nephropathy. • Tubular casts- combination of Bence Jones protein &Tamm-Horsfall protein-obstruct the tubular lumina;induce inflammatory reaction.around the casts. • Amyloidosis-AL type. • Casts-pink to blue amorphous masses, fill & distend the lumen. Giant cell reaction.