Download
1 / 10
100 likes | 105 Views
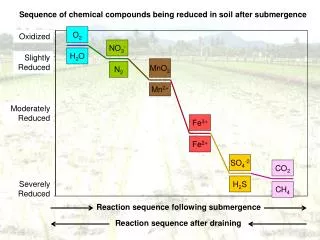
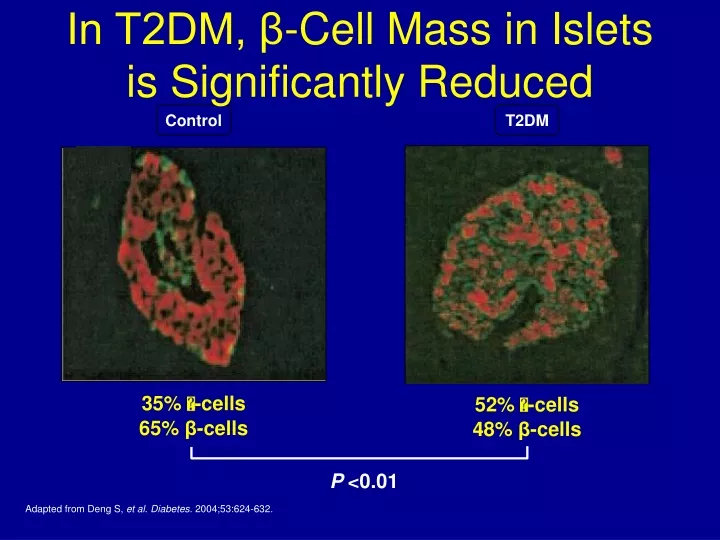
In T2DM, β-Cell Mass in Islets is Significantly Reduced. Control. T2DM. 35% -cells 65% β -cells. 52% -cells 48% β -cells. P <0.01. Adapted from Deng S, et al . Diabetes. 2004;53:624-632. So ‘ maybe ’ Insulin need in T2DM overstated Phenotypic Presentation is defined by :.

E N D
In T2DM, β-Cell Mass in Islets is Significantly Reduced Control T2DM 35% -cells 65% β-cells 52% -cells 48% β-cells P <0.01 Adapted from Deng S, et al. Diabetes. 2004;53:624-632.
So ‘maybe’ Insulin need in T2DM overstated Phenotypic Presentation is defined by: Slope = ‘Natural History’ over time,i.e.,RATE OF β-cell LOSS. Slope is not linear in either T1DM or T2DM, and may be intermittently relapsing, remitting, stabilized, and improved. Complete loss of β-cell mass may never be reached, especially if newer agents better preserve β-cells. 100% − − − − − − − − − 0%− Severity= β-cell loss of mass Beta cell mass is a function of relative rates of apoptosis, replication and neogenesis Pre-Diabetes= FBS ≥100, PPG ≥140 All DM= FBS ≥126, PPG ≥200 Critical β−Cell Mass % β−Cell Mass Disease Modification I I I I I/ ≈ / I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I Increasing Age Age at presentation = tipping point when the combined gene effect / environmental trigger is exposed as phenotypic hyperglycemia
DURABILITY OF GLYCEMIC CONTROL WITH SULFONYLUREAS 1 Glyburide Glyburide Glimepiride SU Glyburide 0 Alvarsson (n=39) GLY SU Alvarsson (n=48) Gliclazide RECORD (n=272) Glyburide Change in HbA1c (%) Hanefeld (n=250) Charbonnel (n=313) -1 Gliclazide UKPDS (n=1,573) Chicago (n=230) ADOPT (n=1,441) PERISCOPE (n=181) Tan (n=297) -2 0 1 2 3 4 5 6 10 TIME (years)
Natural History- Usual ‘Story’- Progressive Loss of Mass Requiring Insulin Therapy in Many/Most- a Myth 1. Progressive Decline in Function – multiple causes of b-cell damage- decreased function>mass- worse with with SU/ Insulin TX BUT 2. Med School- need to do 80% pancreatectomy to become diabetic 3. “..no more than 20-25% of pancreas needed to stay normal after distal pancreatectomy (King-from ref. below ) 4. After Bariatric surgery- even 20 years DM, 15 on insulin- 3 days later no need for insulin, Or , often, on no anti-dm medicine at all So.. Have more b-cells after years than most believe So.. No Sulfonylurea- destroys b-cells; Delay Insulin- avoid effects of hyperinsulinism- hypo- wt.gain Use agents that preserve B-cell function (DeFronzo’s Triple Therapy) -and may decrease CV outcomes So.. No need for early insulin If need insulin- one can avoid bolus in most !! . J Gastrointest Surg (2008) 12:1548–1553,Distal Pancreatectomy: Incidence of Postoperative Diabetes Jonathan King & Kevork Kazanjian & J. Matsumoto & Howard A. Reber & Michael W. Yeh & O. Joe Hines & Guido Eibl
NOTE:There is NO perfect Exogenous Insulin:All result in HyperInsulinemia and Potential Hypoglycemia Exquisitely controlled levels of insulin released into the portal vein Fine-tuned, physiologically appropriate insulinemia Endogenous Insulin ‘Obligatory’ excess peripheral insulin to get modicum of reduced hepatic glucose production Exogenous Insulin Insulin Resistance β-cell Dysfunction ------- Potential β-cell Exhaustion Hypoglycemia Obesity Hyperinsulin-emia Atherosclerosis Weight gain Hypertension Dyslipidemia Cancer Chronic Inflammation Type II Diabetes
Avoid Early Insulin Therapy (except in Ketosis-prone)Vicious Circle(s) of Hyperinsulinemia-Result in Weight Gain and Hypoglycemia Blood glucose rises Undue Basal Or bolus Insulin =Overinsulinized Patient eats too much Or simple sugars Hypoglycemia Symptomatic or not! INCREASED APPETITE
ORIGIN TRIALWith Early Insulin TherapyNo Benefit in reducing Adverse CV Outcomesand increased hypoglycemia and wt. gain
Increased Mortality, MACE, Cancer 1-year After Starting insulin- 2014 Diabetes Obes Metab. 2014 Nov 14. doi: 10.1111/dom.12412. [Epub ahead of print] Glucose-lowering with exogenous insulin monotherapy in type 2 diabetes: dose association with all-causemortality, cardiovascular events and cancer. Holden SE1, Jenkins-Jones S, Morgan CL, Schernthaner G, Currie CJ.
Value to Early Insulin Therapy-Outweighed By Hypoglycemia Weight Gain….