Download
1 / 22
311 likes | 984 Views
Topical Steroid Therapy. Val Anderson Dermatology Specialist Nurse South Gloucestershire Community Health Services. What are steroids?. Essentially hormones Glucocorticoids/ mineralcorticoids Naturally formed in the adrenal cortex

E N D
Topical Steroid Therapy Val Anderson Dermatology Specialist Nurse South Gloucestershire Community Health Services
What are steroids? • Essentially hormones • Glucocorticoids/ mineralcorticoids • Naturally formed in the adrenal cortex • Natural glucocorticoids maintain normal blood sugar and assist the body to recover in times of stress.
Why Topical Steroids ? • To gain control of signs and symptoms of inflammatory skin disease • Achieve maximum efficacy with minimal side effects.
Action of Topical Steroids • Anti-inflammatory • Immunosuppressive • Vasoconstrictive • Anti-mitotic – decrease proliferation • Readily penetrate the dermis “Reduce inflammation and make the skin less sore and itchy”
Steroid Phobia • Present in health care professionals, patients and carers. • A reluctance to use prescribed topical steroids due to perceived side effects • Reassurance is essential to gain full concordance with treatment. REMEMBER: Appropriate topical steroid use limits potential side effects almost entirely.
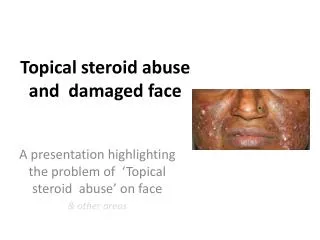
Potential side effects Cutaneous Thinning / Atrophy Hypopigmentation Striae Telangietasia Tachyphylaxis, Infections, Perioral dermatitis, Contact dermatitis, Hirsutism, Monomorphic acne or rosacea N.B Epidermal thinning does occur within 1-3 weeks of tx with potent or very potent steroids normal skin but reverses within 4 weeks of stopping
Potential Side Effects : systemic • These are RARE and ALWAYS AVOIDABLE • Due to systemic absorption of the steroid
Adverse effects : systemically • Osteoporosis • Muscle atrophy • Cushings Syndrome • Inhibition of growth (children) • Cataracts • Masking of infection • Hypoglycaemia
Which steroid?- factors to consider • Age /potency – adult, adolescent or child • Site – absorption increased at certain sites • Extent- localised or generalised • Base- creams or ointments? • Method- frequency of application / occlusion • Experience of use - dexterity
Steroid potencies Group I. Mild e.g. Hydrocortisone 1% OTC (over the counter) Group II. Mod (1 X OTC) Group III. Potent prescription only Group IV. Very potent prescription only Relative potencies compared to Hydrocortisone 1% (Grp I) Group 2 - 2.5 x stronger Group 3 - 10 x stronger Group 4 - 50 x stronger
Steroid application Reassure - explain rationale for use and benefits Early use - to control exacerbations Therapeutic dose - < prolongs flare and subsequent control Demonstrate - light smear, F.T.U (finger tip unit)
Weekly Quantities of steroid Adult using b.d applications Creams and Ointments face & neck…………………… 15 - 30g both hands…………………… 15 - 30g scalp………………………….. 15 - 30g both arms…………………….. 30 - 60g both legs……………………… 100g trunk…………………………... 100g groins & genitalia……………. 15 - 30g BNF March 2006
Summary of NICE Guidelines • No statistical difference between once and twice daily steroid applicaton frequency on efficacy. • Application 10-14 days and consider steroid holiday • Improve patient and carer education
Steroid Workshop Practice finger tip unit measurements Discuss photos and case studies
Case Study 1 • 6 month old baby with history of eczema since 4 months old. • Tried emollients and has been given topical steroids by GP 2 weeks ago. • O/E moderate eczema present on facial cheeks. Excoriations present and baby waking at night. • Not improved since prescription for topical steroid given.
What issues related to topical steroid use would you consider during assessment and treatment decisions for this child ?
Case Study 2 • 14 year old boy • History of eczema since 2 years old. • O/E has moderate levels of eczema in arm flexures with some weeping. • Prescribed hydrocortisone 1% ointment by GP 3 weeks ago- nil improvement. • Arms now becoming sore.
What issues related to topical steroid use would you consider during assessment and treatment decisions for this child ?