Download
1 / 40
410 likes | 942 Views
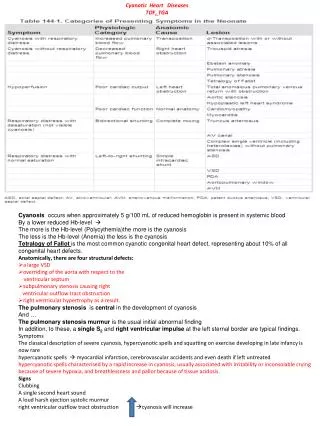
Cyanotic Heart Lesions. Neonatal Intensive Care Nursery Night Curriculum Series. Cyanosis. Arterial saturation less than 90% and a PO 2 less than 60 torr In all cyanotic heart lesions the amount of cyanosis seen is dependent on the amount of pulm blood flow Decreased PBF- increased cyanosis

E N D
Cyanotic Heart Lesions Neonatal Intensive Care Nursery Night Curriculum Series
Cyanosis • Arterial saturation less than 90% and a PO2 less than 60 torr • In all cyanotic heart lesions the amount of cyanosis seen is dependent on the amount of pulm blood flow • Decreased PBF- increased cyanosis • Increased PBF- minimal cyanosis but CHF may develop • With 100% oxygen • PO2 >250 is not congenital heart disease • PO2 <100 is cardiac disease
5 “T’s” • Most common cyanotic lesions of the newborn • Tetralogy of Fallot • Transposition of the Great Arteries • Truncus Arteriosus • Total Anomalous Venous Return • Tricuspid Atresia
PGE • For cyanotic heart lesions with reduced blood flow • RE-opens PDA and prevents it from closing • Allows partially desaturated systemic arterial blood to enter the pulmonary artery and be oxygenated • Initial dose 0.1mg/kg/min • Side effects- apnea, fever, hypotension
Complete Transposition of the Great Arteries • 5% of all CHD • Boys 3:1 • Most common cyanotic condition that requires hospitalization in the first two weeks of life
Complete Transposition of the Great Arteries • Aorta arises from the right ventricle • Pulmonary artery arises from the left ventricle
Complete Transposition of the Great Arteries • Complete separation of the 2 circuits • Hypoxemic blood circulating in the body • Hyperoxemic blood circulating in the pulmonary circuit
Complete Transposition of the Great Arteries • Defect to permit mixing of 2 circulations- ASD, VSD, PDA. • VSD is present in 40% of cases • Necessary for survival
Clinical Symptoms • Depend on anatomy present • No mixing lesion and restrictive PFO • Profound hypoxia • Rapid deterioration • Death in first hours of life • Absent respiratory symptoms or limited to tachypnea • Single second heart sound, no murmurs
Clinical Symptoms • Mixing lesion present (VSD or large PDA) • Large vigorous infant • Cyanotic • Little to no resp distress • Most likely to develop CHF in first 3-4 months of life • excessive sweating (a cold, clammy sweat often noted during feeding); poor feeding, slow weight gain, irritability or lethargy, and/or rapid breathing
CXR • Egg shaped cardiac silhouette • Narrow superior mediastinum
Management • Prostaglandin to establish patency of the ductus arteriosus • Increases shunting from aorta into the pulmonary artery • Increases pulmonary venous return distending the left atrium • Facilitates shunting from the left to the right atrium of fully saturated blood across the foramen ovale.
Management • Therapeutic balloon atrial septostomy (Rashkind Procedure) if surgery is not going to be performed immediately • Improves mixing and pulmonary venous return at the atrial level
Treatment • Surgery consists of switching the right and left sided structures at the atrial level, at the ventricular level, or at the great artery level.
Tetraology of Fallot • VSD • RVOT Obstruction • RVH • Overriding aorta
Two Important Abnormalities • NonRestrictive VSD • Large enough to equalize pressures in both ventricles • Degree of RVOT
Clinical Presentation of Cyanotic TOF • Cyanosis, clubbing, dyspnea on exertion, squatting, hypoxic spells. • Loud systolic ejection murmur, systolic thrill at middle LSB • Soft murmurs are associated with less blood flow and more hypoxia
Hypoxic Spell (“TET Spell”) • Peak incidence of 2-4 months • Characterized by: • Hyperapnea (Rapid and deep respirations) • Irritability and prolonged crying • Inc cyanosis • Decreased heart murmur
Pathophysiology • Lower SVR or inc resistance of RVOT can increase the R-L shunt • Stimulates the respiratory center to produce hyperapnea • Results in an increase in systemic venous return • In turn, increases R-L shunt through VSD
TET Spell Treatment • Hold infant in knee-chest position • Morphine • Sodium bicarbonate to treat acidosis- decreases resp stimulating effect of acidosis • Vasoconstrictor (phenylephrine) • Propranolol
Treatment • Early surgical repair depending on pt’s weight • VSD is closed and obstructing ventricular muscle is removed
Total Anomalous Pulmonary Venous Return • The pulmonary veins drain into the RA or its venous tributaries rather than the LA • A interatrial communication (ASD or PFO) is necessary for survival • Pulmonary venous return reaches the RA • Systemic and pulmonary venous blood are completely mixed
4 Types 1. Supracardiac Common pulmonary vein drains into the SVC via the left SVC and left innominate vein.
2. Cardiac • The common PV drains into the coronary sinus
3. Infracardiac • The common PV drains into the portal vein, ductous venosus, hepatic vein, or IVC. Infracardiac-type TAPVC. Pulmonary venous blood draining through the liver to reach the IVC and right atrium.
4. Mixed • A combination of the other types
Clinical Signs for Unobstructed Veins • Mild cyanosis, signs of CHF in infancy, history of pneumonia • Widely split S2, Grade 2-3/6 systolic murmur heard at the ULSB • CXR- marked cardiomegaly
Clinical Signs for Obstructed Veins • Profound desaturation • Acidosis • PGE1 administration does not improve oxygenation because elevated pulmonary pressures in the right side of the heart (due to obstructed pulmonary outflow) will result in right to left shunting across an open ductus further decreasing arterial saturation.
Treatment • Digitalis and diuretics to treat heart failure • Intubation and inc PEEP for those with severe pulm over load • Corrective surgery
Tricuspid Atresia • Tricuspid valve is absent • RV and PA are hypoplastic • Associated defects- ASD, VSD, or PDA (necessary for survival) • Dilation of LA and LV • Essentially single ventricle physiology
Clinical Signs • Severe cyanosis, poor feeding, tachypnea • Single S2, grade 3/6 systolic murmur at LLSB if VSD is present • CXR- boot shaped heart
Treatment • PGE IV infusion • Blalock-Taussigshunt in infancy • systemic to pulmonary arterial shunt • Provide stable blood flow to the lungs • A gortex tube is sewenbetween the subclavian artery and the right pulmonary artery
Bidirectional Glenn • Superior vena cava is connected to the pulmonary arteries • IVC continues to be connected to the heart
Fontan Procedure • Redirects IVC to lungs
TruncusArteriosus • A single trunk leaves the heart • Gives rise to pulm, systemic, and coronary circulations • Large VSD is always present
Clinical Signs • Cyanosis immediately after birth • Early signs of CHF • 2-4/6 systolic murmur at LSB suggestive of VSD
Treatment • Anticongestive medications (diuretics and digitalis) • Corrective surgery • VSD is closed • Pulmonary artery is separated from the truncus • Continuity is then established between the right ventricle and the pulmonary artery utilizing a valved homograft conduit