Download
1 / 39
390 likes | 514 Views
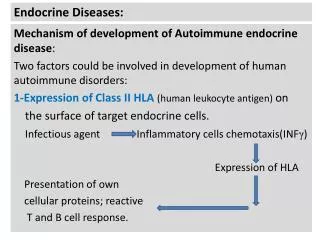
Endocrine disorders & Steroid Therapy Dental Overview. Adrenal Gland. Adrenal Gland. Cortex Zona glomerulosa Aldosterone Zona fasciculata Cortisol Zona reticularis Sex hormones Medulla Cathecolamines (Epinephrine)

E N D
Adrenal Gland • Cortex • Zona glomerulosa Aldosterone • Zona fasciculata Cortisol • Zona reticularis Sex hormones • Medulla Cathecolamines (Epinephrine) • Glucocorticoids (cortisol): essential for metabolism, anti-inflammatory, homeostasis during stress • Mineralocorticoids (aldosterone): fluid, sodium and potassium balance • Androgens
Adrenal Gland Physiology Stress stimulates the hypothalamus to secrete CRH CRH stimulates the pituitary to produce ACTH ACTH stimulates the adrenal cortex to produce cortisol Cortisol level increases within minutes after stimulation
Hormones produced by adrenal cortex: Cortisol Aldosterone Sex hormones (androgens) Syndromes: Cushing Syndrome Hyperaldosteronism (Conn syndrome) Adrenogenital (virilizing) syndromes Adrenocortical Hyperfunction
Cushing Syndrome Endogenous • Pituitary hypersecretion of ACTH • Adrenal hypersecretion of cortisol (adenoma, carcinoma, nodular hyperplasia) • Ectopic ACTH (small cell lung cancer) Exogenous (Cushing syndrome ) 4. Administration of exogenous glucocorticoids
Cushing Syndrome – Clinical Features • Hypertension • Weight gain: • Truncal obesity • “moon” face • “buffalo hump” • Decreased muscle mass • Hyperglycemia • Catabolic effect on proteins with loss of collagen: cutaneous striae, easy brusing, osteoporosis • Hirsutism, amenorrhea • Increased risk of infections (because of decreased immune response)
Only ACTH producing etiologies are associated with coloration changes due to the stimulation of melanocytes by ACTH. Skin atrophy
Adrenocortical Insufficiency • Acute • Massive adrenal hemorrhage (DIC, sepsis = Waterhouse-Friderichsen syndrome.) • Sudden withdrawal of long-term corticosteroid therapy • Stress in patients with chronic adrenocortical insufficiency • Chronic (Addison disease) • Autoimmune, infections (TB, fungal), AIDS, metastatic cancers
Addison disease : Clinical features: Progressive Weakness Fatigue Weight loss Inability to tolerate stress GI symptoms: anorexia, vomiting, weight loss Hyperpigmentation (ACTH stimulates melanocytes ) Low aldosterone: hyponatremia, hypovolemia , hypotension hyperkalemia , acidosis Low cortisol: hypoglycemia Death if untreated
Oral manifestations/ dental aspects: Diffuse patchy brown macular pigmentation of the oral mucosa Consider steroid cover before treatment
Adrenal Crisis(Acute Adrenal Insufficiency) • Hypotension • Severe weakness • Progressive mental confusion • Nausea and vomiting • Abdominal, lower back or leg pain • Hyperthermia • Hypoglycemia • Hyperkalemia • Improve CAD • Loss of consciousness • Coma • death
Adrenal Crisis Weight Loss Fatigue Weakness Severe Hypotension Abdominal Symptoms
Management of Corticosteroid-use Dental PatientsPrevent Adrenal Crisis
Hydrocortisone 100mg Dexamethasone 5mg Management of Acute Adrenal Insufficiency: • Terminate all procedures • Supine position with leg elevation • Administer hydrocortisone 100~200mg or Decardron 5~10mg • Administer O2 • Monitor vital signs • Set up IV line • Start BLS if indicated • Transportation to a medical facility as soon as possible
Dental Management of the Patient Taking Corticosteroids Routine procedures (excluding surgery) a. Good local anesthesia & postoperative pain control if necessary b. Monitor blood pressure during procedure Dental extractions or surgery a. Corticosteroid dose generally will need to be increased, consult patient’s MD prior to the procedure • Dental aspects: • Steroid cover in the “syndrome” cases • Complications
Hyperaldosteronism • Na retention and K excretion HTN, hypokalemia • Primary (Conn syndrome) • Adrenal cortical adenoma • Suppression of RAA: plasma renin = low • Secondary • Due to decreased renal perfusion (renal artery stenosis, arteriolar nephrosclerosis, CHF) • Activation of RAA: plasma renin = high
Functions of Corticosteroid • Regulation of carbohydrate, fat, protein • Anti-inflammation action by inhibit lysosome, prostaglandin, cytokines release. • Regulate the function of leucocyte. • Increase gluconeogenic, proteolysis, lipolysis and blood sugar
Clinical Application of Steriod • Immunosuppressive: Rheumatoid arthritis, SLE, organ transplantation, asthma… • Anti-inflammation: hepatitis, dermatoses, mucositis, post-op edema… • Analgesia: reduction of pain • Replacement for Adrenal Insufficiency
Adverse effect of Corticosteroids • Receive long-term, high-dose steroid • Hypertension, heart failure • Osteoporosis, DM, impaired wound healing, mental depression and psychosis • Peptic ulcer, Cataract, glaucoma, growth suppression, hypocalcemia, PTH increased • Cushing syndrome • Secondary adrenal insufficiency
Dental uses of Corticosteroids • Topical use: non-infections, ulcerative diseases in oral cavity. Inhibit the inflammatory reaction, redness and edema • Systemic use: Pre-prosthetic surgery, Reconstructive oral surgery & surgery
Condition Administration
Dental patient taking Steroid Supplementation NOT required • Patient taking low dose (<20 mg of cortisol daily) • Patient taking large dose: For less than 2 weeks For minor dental procedure with minimal stress
Dental patient taking Steroid Supplementation Required • Patient taking large dose: for greater than 2 weeks for extensive major or stressful dental procedure # Double usual daily dose on the day before, the day of, and the day after surgery # Appointment in the morning # Good pain control # Resume normal maintenance dose post-op 2 days.
Dental patient taking Steroid supplementation Required • If the patient received at least 20mg of cortisol for more than 2 weeks within past year #60mg cortisol (or equivalent) the day before and the day of surgery at morning # On first 2 post-op days, 40mg cortisol # Then take 20mg cortisol thereafter, until post-op 6 days.