Download

1 / 51
510 likes | 708 Views
The Integrative Management of Neurodegenerative Disorders – Nutritional Perspective. 神經內科 張嘉祐 醫師. Neurodegenerative diseases. Neurodegenerative Diseases ( Alzheimer's Disease, Parkinson's Disease, amyotrophic lateral sclerosis (ALS), prion diseases,

E N D
The Integrative Management of Neurodegenerative Disorders – Nutritional Perspective 神經內科 張嘉祐 醫師
Neurodegenerative diseases • Neurodegenerative Diseases • ( Alzheimer's Disease, Parkinson's • Disease, amyotrophic lateral • sclerosis (ALS), prion diseases, • frontotemporal dementia (FTD), and • Huntington's Disease.) • Age-related disorders
Cancer, cerebrovascular disease, and • heart disease account 75% of all death • of age 65 and older. • Neurodegenerative pathologies such as • Alzheimer’s disease will increase and • become a significant cause of mortality. • Senile dementia increase 24 % between • 2000 to 2010 and 26 % between 2010 to • 2020 • It costs about $ 60 billion a year to care • for AD patients. If we could delay the • onset by just 5 years, we could cut that • cost in half.
It is not aging to which many neurological signs should be attributed, but rather to the neurodegenerative syndromes that accompany aging.
慢 性 病 生活習慣病 日野原重明
飲食 遺傳 生活型態 老化 生活型態 壓力 心理
SIGNS SYMPTOMS MEDIATORS TRIGGERS DIATHESIS & ANTECEDENTS Patient Centered Assessment
Diathesis and Antecedents • Every aspect of the patient’s life that may have predisposed him or her toward an illness is gathered together under the concept of diathesis. • Personal and individual (biochemical individuality, genetic uniqueness)
Genotype VS Phenotype
Basic points about genes • Your genes are unique and not identical to anyone else’s even if you are an identical twins. • All the genetic messages you need to remark yourself are present in every cell of your body. • At any one time some genes are being expressed and others are not. • Genetic messages may be partially expressed. • You can modify the expression of many genes through diet, nutrients, exercise, life style and environment.
Triggers and Mediators • Triggersmay be located either inside (endogenous) or outside(exogenous) the body. • Triggers include exposure to microbes (viruses, bacteria, parasites, etc) and exposure to specific food or food components like lectins or antigens. • Mediators are always inside the body . • Hormones, neurotrasmitters, reactive oxygen species, cytokines, kinins, eicosanoids, and ions are important mediators
PATIENT WORKUP Nutritional Status Immune/Inflammation Oxidative stress GI Function Detoxification Structural Neuro-Endocrine Mind-Body
Xenobiotics Drugs Alcohol Apoptosis Oxidant stress and mitochondrial damage ApoE, cytokines GI permeability Immune Cells “dysbiosis” NO/alteration of detoxification Airborne pollutants
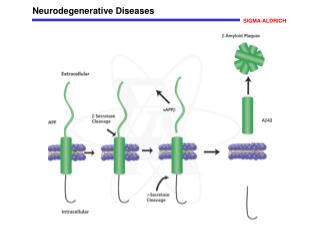
Alzheimer’s disease -pathology • The neuropathological hallmarks of neurofibrillary tangles and senile plaques were described by a German psychiatrist, Alois Alzheimer, in 1907 • Senile (neuritic) plaques result from the accumulation of several proteins and an inflammatory reaction around deposits of b-amyloid
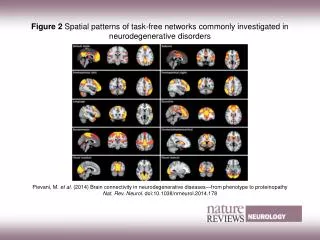
Mechanisms of Neurodegenerative Disorders – Protein Aggregates
Commonalities between genetics of cardiovascular disease andneurodegenerative disorders Current Opinion in Lipidology 2004, 15:121–127 • The intensive search conducted in the past • year gave rise to many publications, more • than half of which were related to genes • common to cardiovascular and • neurodegenerative disorders. • The majority of the genes studied are • involved in cholesterol metabolism, • hypertension, lipid oxidation and detoxication • or inflammatory processes.
Atorvastatin for the Treatmentof Mild to Moderate Alzheimer DiseasePreliminary ResultsArch Neurol. 2005;62:753-757 • Epidemiological studies suggest that prior statin use in treating risk of coronary artery disease may reduce the risk of AD later in life. • Atorvastatin reduced circulating cholesterol levels and produced a positive signal on each of the clinical outcome measures compared with placebo.
Apolipoprotein E (APOE), the susceptibility gene • locus for late-onset (55 and older) AD affecting the • risk and age of onset distribution in the population • APOE has three common alleles, designated e2, e3, • and e4 . • Familial late-onset AD, the e4 allele frequency was • found to be 0.50, compared to 0.16 for age-matched • controls. • Saunders et al then looked at a very large series of • 176 autopsy-confirmed sporadic patients with AD • who had the clinical syndrome and pathological • confirmation, but no known family history . The e4 • allele frequency in this sporadic series was 0.40, highly • significantly different from controls.
ApoE and Abeta 1-42 interactions: effects of isoform and conformation on structure and function. J Mol Neurosci. 2004;23(3):235-46. . • The hypothesis is that apoE has two general • functions in relation to A beta : • First, apoE interacts with oligomeric A beta via • an apoE receptor-mediated process to inhibit • neurotoxicity and neuroinflammation (apoE3 > • apoE4) a process possibly related to binding and • clearance of apoE3:oligomer complexes. • Second, apoE facilitates the deposition of A beta • as amyloid (apoE4 > apoE3).
Inflammatory molecules and mechanisms are uniquely present or significant elevated in the AD brain • Inflammation may be a necessary component of AD pathogenesis • Inflammation may be sufficient to cause AD neurodegeneration. • Retrospective and direct trials suggest a therapeutic benefit of conventional antiinflammatory medications in slowing the progress or even delaying the onset of AD
Effect of non-steroidal anti-inflammatory drugs on risk of Alzheimer's disease: systematic review and meta-analysis of observational studies BMJ. 2003 Jul 19;327(7407):128 • The pooled relative risk of Alzheimer's disease among users of • NSAIDs was 0.72 (95% confidence interval 0.56 to 0.94). • The risk was 0.95 (0.70 to 1.29) among short term users (< 1 • month) • 0.83 (0.65 to 1.06) among intermediate term (mostly < 24 • months) • 0.27 (0.13 to 0.58) among long term (mostly > 24 months) users . • The pooled relative risk in the eight studies of aspirin users was • 0.87 (0.70 to 1.07). • NSAIDs offer some protection against the development of • Alzheimer's disease. The appropriate dosage and duration of • drug use and the ratios of risk to benefit are still unclear.
The influence of systemic inflammation on inflammation in the brain: implications for chronic neurodegenerative disease. Perry VH. Brain Behav Immun. 2004 Sep;18(5):407-13 • Systemic inflammation may impact on local • inflammation in the diseased brain leading to • exaggerated synthesis of inflammatory cytokines and • other mediators in the brain, which may in turn influence • behaviour. • Systemic infections, or indeed any systemic challenge • that promotes a systemic inflammatory response, may • contribute to the outcome or progression of chronic • neurodegenerative disease.
The incidence of Alzheimer’s disease is highest in carriers of the apolipoprotein (APO) E-ε4 allele who harbour HSV-1 DNA in the CNS, so it is possible that these agents are co-factors for the disease.
Lancet Neurology 2003: 2: 425–28 A recent prospective study (S Seshadri and colleagues N Engl J Med; 2002 346: 476–83) showed hyperhomocysteinaemia to be a strong, independent risk factor for dementia and AD. The researchers found a graded increase in risk of both outcomes with rising plasma concentration of homocysteine after multivariate control for putative risk factors for AD.
A placebo-controlled, double-blind randomized trial of an extract of Ginkgo biloba for dementia Le Bars, P JAMA October 22, 1997 • 137 patients, 52 weeks, Egb 120mg/d • 27 % treated group improved on standardized cognitive testing • Egb actions: homeostasis of inflammation, membrane protection, neurotransmission modulation
The use of melatonin in Alzheimer's disease Neuro Endocrinol Lett. 2002 ;23 Suppl 1:20-3 • Melatonin improved sleep and suppressed • sundowning agitation, an effect seen • regardless of the concomitant medication • employed to treat cognitive or behavioral • signs of AD. • Melatonin treatment seems to constitute • a selection therapy to ameliorate sundowning • and to slow evolution of cognitive impairment in • AD patients. • Metatonin has the capacity to interchelate into b- • pleated sheet structures and break them up. • Melatonin is also an antioxidants.
Curcumin (薑黃) inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo J Biol Chem. 2005 280(7):5892-901 • The phenolic yellow curry pigment curcumin has • potent anti-inflammatory and antioxidant • activities • Curcumin was a better A beta 40 aggregation • inhibitor than ibuprofen and naproxen • Curcumin directly binds small beta-amyloid • species to block aggregation and fibril formation • in vitro and in vivo.
Prevention of Alzheimer’s disease: Omega-3 fatty acid and phenolic anti-oxidant interventions Neurobiology of Aging 26S (2005) S133–S136 • Because of its availability and low cost, coupled with preclinical data showing its potential for intervention at multiple sites inAD pathogenesis, curcumin is now in clinical trials in mild to moderate AD patients under an FDA approved IND by theUCLA Alzheimer Center • Epidemiology shows risk reduction of 60% associated with modest increases in DHA intake or plasma levels. DHA works well in slowing AD pathogenesis in mice with a human AD gene and is safe enough to include in infant formula. It should be a strong candidate for use in primary prevention.
A Broad Spectrum of Potential Etiologic Factors • Role of Aging • Heritability and Genetic • Susceptibilities • Environmental Contributors, • Especially Toxins
Genetically determined differences in Xenobiotic metabolism as a risk factor in Parkinson’s diseaseFundam appl Toxicol, 1996 (30) • Patients with inherited CYP2D6 ,Non- inducible genetic polymorphism (10% poor metabolizers) , cytochrome P450 enzyme deficiency had 2.4 X increased risk for Parkinson’s disease
Xenobiotic metabolism in Parkinson’s diseaseNeurology, July, 1989 • Severe deficiency of sulfate conjugation in 70 % of PD subjects • PD may be unusually susceptible to exogenous or even endogenous toxins
長期暴露農藥中患巴金森氏症風險增加 記者江志雄╱羅東報導巴金森氏症是老人常見腦神經退化疾病之一,國內一項針對一百二十五名老年巴金森氏症患者進行之研究發現,長期大量暴露在農藥中,可能與罹患巴金森氏症有關,且暴露時間越長,罹病風險越高。過去香港也有研究指出,有長期農藥暴露史者,罹病風險將提高三點六倍,德國也曾有類似報告。 自由時報九十四年七月二十二日
Xenobiotics Drugs Alcohol Apoptosis Oxidant stress and mitochondrial damage ApoE, cytokines GI permeability Immune Cells “dysbiosis” NO/alteration of detoxification Airborne pollutants
Complex Problems, Simple Solutions
Food is the best medicine • There is no substitute for a healthy, well-balanced • diet. Supplements can help enhance the health • benefits of food, but they cannot do the Job. • Many of the important phytochemicals are in the • pigments of plants. • Fresh whole fruits and vegetables are your best • option. • There is no magic bullet. Different phytochemicals • work together to achieve their effects. • Limit fat consumption to around 30 percent of • your daily calories. raw, unhydrogenated oils, • such as canola oil, olive oil, flaxseed oil, and • peanut oil are the healthiest.
Morning Counts as13/4 cup Counts as1medium-size Mid-day Counts as1medium-size Counts as22 cups Evening Counts as11/2 cup Counts as21 cup Counts as11/2
飲食 遺傳 生活型態 生活型態 壓力 心理