Download
1 / 36
360 likes | 364 Views
Learn how to safeguard and promote the welfare of children, identifying signs of abuse and reporting concerns. Understand the assessment framework and the concept of significant harm.

E N D
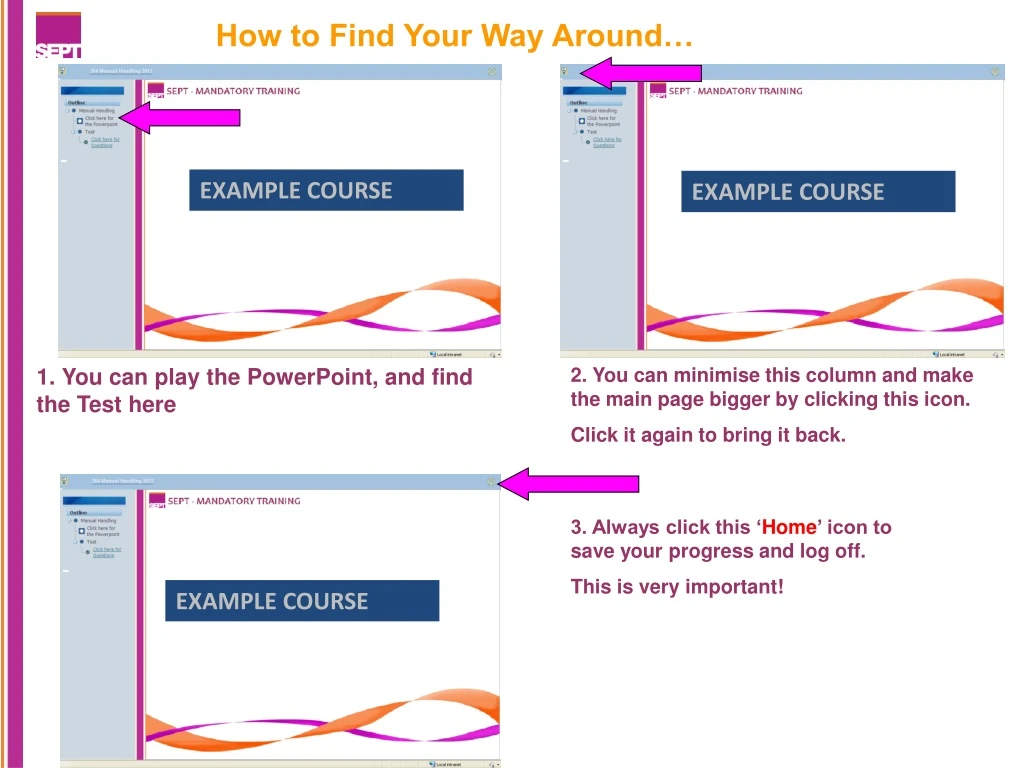
EXAMPLE COURSE EXAMPLE COURSE How to Find Your Way Around… 1. You can play the PowerPoint, and find the Test here 2. You can minimise this column and make the main page bigger by clicking this icon. Click it again to bring it back. 3. Always click this ‘Home’ icon to save your progress and log off. This is very important! EXAMPLE COURSE
Safeguarding children is everyone's responsibility. All staff have a statutory duty to report concerns, allegations or direct disclosures regarding a child's welfare to their Line Manager and/or the Safeguarding Children Team. Reports of concerns may come from other staff or by direct disclosure or information from the child’s family, friends or neighbours. Safeguarding and promoting the welfare of children and young people Safeguarding and promoting the welfare of children is defined as protecting children from maltreatment, preventing impairment of children’s health and development and ensuring children have optimum life chances. A 'child' is anyone up to their eighteenth birthday.
The Children Act 1989 (Section 17) The Children Act 1989 (section 17) defines a child in need; as children or young people who because of their vulnerability, will need the provision of services in order to reach or maintain a satisfactory level of health or development Where a child in need is identified, practitioners working with the child will complete a Common Assessment Framework (CAF) which may then be forwarded to a local multi agency group for a co-ordinated response and delivery of services to the child/young person and their family. The assessment triangle is a tool for staff to use when making a holistic assessment of the child and family. Consent from the parent and/or young person is central to this process.
Assessment Framework Triangle Health Education Identity Family & Social Relationships Social Presentation Emotional & Behavioural Development Self-care Skills Social Presentation Basic Care Ensuring Safety Emotional Warmth Stimulation Guidance & Boundaries Stability Child and Development Needs Parenting Capacity CHILD Safeguarding & Promoting Welfare Family and Environmental Factors Family History & Functioning, Wider Family, Housing, Employment, Income, Family’s Social, Integration, Social Resources
The Children Act 1989 (section 47) The Children Act 1989 (section 47) introduced the concept of significant harm as a definition of abuse; harm means ill treatment or the impairment of health or development including impairment from seeing or hearing the ill treatment of another. Significant relates to the child’s health and development and the comparison with that which could reasonably be expected of a similar child. Where a child or young person has been identified as at risk of significant harm the Local Authority (Social Care) has a legal duty to make enquiries and take appropriate action to ensure the safety of the child/young person. Consent for these enquiries is not obligatory, but agencies will always seek to work with parents where this does not place the child or young person at increased risk.
Abusers come from all walks of life Abuse can occur within the family, an institution or community setting. Abuse can occur in all social groups regardless of age, gender, race, religion, culture, social class or financial position. Children may be abused by: Someone the child knows well who may also be in a position of trust or power or more rarely a stranger. By an Adult(s) By a child/young person All staff who work with children or adults from any service have a responsibility in safeguarding children when they become aware of or identify a child at risk of harm. This includes considering the implications for children of parents’ or users’ behaviours and the impact these may have on their parenting capacity.
Child abuse can take many forms, but is usually divided into four categories. Physical Abuse Involves a range of physical injuries including hitting, shaking, throwing, poisoning, burning, scalding, drowning or suffocating and also includes fabricated and/or induced illness. Signs that could indicate physical abuse include: Bruising is more likely to be non accidental if: On a non-mobile baby or child (maybe non mobile because of age or disability) On any fleshy, non-bony part of the body, for example: face, neck, buttocks or back Multiple bruising or clusters e.g. finger prints Bruises with a defined outline Bruises are more likely to be accidental when found on the bony prominences of the body for example: forehead, chin, knees, shin, back of head Fabricated or Induced Illness is classed as a physical abuse where a parent/carer fabricates or deliberately induces illness in a child
Burns & Scalds Burns include scalds from hot liquids, contact burns from hot objects (such as an iron) burns caused by flames, chemical and electrical. Burns with a clear outline or uniform depth for example may be more indicative of non accidental injury. Most burns are accidental. A recent UK study estimates that of the children admitted to burns units, 10% had sustained burns that were the result of abuse and burns due to neglect outnumber intentional burns by a ratio of nine to one. Any injury which the child, parent, carer tries to hide or give several different or unlikely explanations, should raise concerns. In these circumstances advice should always be sought. Bites Bites can leave a clear impression and abuse should be considered as a possibility especially when is thought unlikely to have been caused by a young child. An animal bite on a child may indicate neglect for example: inadequate supervision of the child or failure to protect from danger.
Sexual Abuse Trust staff must report any known cases to their line manager and the Trust Safeguarding Team and a referral made to Children’s Social Care. It may also be appropriate to contact the Police if the situation is urgent, although social care will always liaise with them Sexual abuse involves forcing or enticing a child or young person to take part in sexual activities, including sexual exploitation whether or not the child is aware of what is happening. This may involve sexual physical contact or non-contact activities including coercing or grooming children by the use of pornographic material or watching sexual activities including those via the internet, webcams, cameras, mobile phones, or encouraging children to behave in sexually inappropriate ways. It is important to recognise that children & young people can be sexually abused by adult males, females and other children & young people ‘I was chatting to a boy who is 15 years old on the MSN this evening. He flashed his private parts to me via webcam. I am scared and worried.’ (Girl aged 9) Two thirds (65.9%) of contact sexual abuse experienced by children aged 0-17 was perpetrated by someone aged under 18 (NSPCC 2011) 7% of all the children subject of a child protection plan in the UK were under a category that includes sexual abuse on 31 March 2010 (NSPCC)
If you are aware of a child that has contact with an adult with prior allegations or convictions of sexual abuse you must seek advice from the Safeguarding team and your line manager with a view to making a child protection referral. A child under 13 years is not legally capable of consenting to sexual activity (The Sexual Offences Act 2003) Sexual activity with a child under 16 years is also an offence, however where it is consensual it may be considered less serious, although there may still be serious consequences for the welfare of the child/young person and consideration about whether there is a need to share information with other agencies in order to protect the child/young person should be given in every case. Wetting and/ or soiling especially where a child has been previously toilet trained Signs which could indicate sexual abuse include: Sexually transmitted disease Children displaying inappropriate sexualised behaviour or language for their age and stage of development Child/Young person has money or gifts that they cannot account for Sexually inappropriate relationships, such as discrepancy in age or position of power or trust Changes in behaviour such as withdrawn, or aggressive, risk taking such as running away or substance misuse Self Harming behaviour, including eating disorders and hair pulling Pregnancy or concealed pregnancy in a young person
Emotional Abuse Emotional abuse may involve a parent or carer: Being emotionally unavailable to the child because of adult behaviours or factors including parental substance misuse, mental ill health or domestic abuse Persistent emotional maltreatment which causes severe and persistent effects on the child or young persons’ emotional development. This can occur where there is persistent emotional unavailability and unresponsiveness from the parent or carer towards a child and in particular towards a baby. Conveying to a child they are worthless or unloved and may include not giving a child the opportunity to express their views, deliberately silencing them or ‘making fun’ of what they say or how they communicate Where there is domestic abuse within the family Using the child for the fulfilment of the adult’s needs (for example, children being used in marital disputes). Imposing age or developmentally inappropriate expectations on a child/young person Rejecting or scapegoating a child or young person. Allowing a child to see or hear the ill treatment of another, including pets and Causing a child to feel frightened or in danger or the exploitation or corruption of a child/young person Behaving in a negative or hostile way towards a child or young person “Mum and Dad split up. Since then I feel like they’ve used me as a go-between in their arguments. Mum and Dad don’t speak to each other and I am expected to pass messages.” Girl, aged 16 NSPCC
An emotionally abused child or young person may present with: Self harming behaviours including eating disorders Some level of emotional abuse is involved in all types of maltreatment of a child or young person, although it may also occur alone Changes in behaviour, clinginess, fearful, withdrawn, attention seeking, constantly seeking to please Depression Low self esteem Increased risk taking behaviour
Neglect Neglect is the persistent failure to meet the child’s basic physical and or psychological needs, likely to result in the serious impairment of the child or young person’s health and/or development. Neglect may occur during pregnancy as a result of maternal substance misuse. Neglect has harmful physical, emotional and social consequences for children and young people and can ultimately be fatal A neglected child or young person may present with: Frequently having ingrained dirt on clothing and body, may smell of urine, faeces or body odour Missing routine health appointments Delayed Development Missing significant amounts of school, including children and young people that are caring for others in the home and are unable to access education and social activity Persistently hungry, may steal food from other children at school Significant dental caries Significant untreated childhood conditions such as head lice infestation, eczema Significantly under or over weight
Provide adequate food, clothing and shelter (including exclusion from home or abandonment) and a clean safe environment Neglect may involve a parent or carer failing to: Ensure adequate supervision including the use of inadequate care givers, or leaving young children home alone Protect a child/young person from physical and emotional harm or danger, including domestic abuse Ensure appropriate access to medical care or treatment, including attending health appointments Ensure children and young people have access to appropriate education These categories overlap and an abused child frequently suffers more than a single type of abuse.
What factors may increase risk to children You should be aware of factors that may affect parenting capacity and impact on a child/young person’s safety and welfare, particularly domestic abuse, parental mental ill health and parental substance misuse. The risk to the child when these factors co-exist is significantly increased Ways in which these factors can impact on parenting capacity include: Neglect of physical needs Neglect of Emotional needs by being emotionally unavailable Parenting skills, a parent may be unpredictable, inconsistent and ineffective with their children Children may be expected to fend for themselves and care for the parent and/or younger siblings
Domestic abuse The Home office defines domestic abuse as “any incident of threatening behaviour, violence or abuse between adults who are or who have been intimate partners or family members, regardless of gender or sexuality” This includes issues of concern to black and minority ethnic (BME) communities such as so called ‘honour based violence, female genital mutilation (FMG) and forced marriage UK evidence suggests domestic abuse is a known issue in 1 in 3 child protection cases. Research indicates a strong link between domestic abuse and other forms of child abuse and also animal cruelty. Facts about domestic abuse: Domestic abuse often starts or escalates when a woman is pregnant Children can be at risk of physical injury including harm to the unborn child, either by direct injury or from attempting to protect the non abusing parent Prolonged and /or regular exposure to domestic abuse can have a serious long term impact on a child’s health, development and emotional wellbeing.
Children and young people may express distress through their behaviours in different ways for example: Display aggressive and bullying behaviour Running away from home Self harming Become involved in substance misuse Become withdrawn and isolated Miss school because they are concerned about what is happening at home Be unable to concentrate on learning or play and begin to fall behind developmentally Have sleep disturbance such as nightmares or bedwetting Become anxious and or depressed “Dad sometimes hits mum when he’s angry. I think it may be my fault because I can never get things right with my dad” Natalie 14 yrs (quote from ChildLine 2007) Two women are killed each week in England and Wales by a partner or former partner, 30% of cases start during pregnancy and 90% of children are in the same or next room when violence occurs (Home Office, 2007). Women living in households where there is Domestic Abuse are at an increased risk when pregnant. Domestic Abuse can affect the unborn child through physical injury, (kicks/punches to the abdomen) stress and anxiety to the mother and a failure to attend ante natal appointments.
Parental drug and alcohol misuse Misuse of drugs (prescribed or illegal) and or alcohol is strongly associated with significant harm to the unborn child, children and young people, evidence shows that when parents have problems with substance misuse this often adversely affects their ability to respond to the needs of their children. Non compliance with treatment, this is also a wider issue which often indicates difficulty parents have with organising their own lives, they may neglect their own needs and in turn neglect the needs of their children. Lives are often chaotic with little regard for routines, boundaries and supervision.
Misuse of drugs (prescribed or illegal) and or alcohol is strongly associated with significant harm to the unborn child, children and young people, especially when combined with other features such as domestic abuse and mental illness. Many of the children who rang ChildLine told us that physical, sexual and emotional abuse and neglect were all linked in their lives with alcohol and drug misuse. This is evidence that the emotional volatility, the reduced ability to parent responsibly and the reduction in normal inhibitors can have the most serious impact on children’s lives (NSPCC 2010) What type of abuse is this? Select the correct answer to continue “My dad broke my nose last year when he was drunk. My sister has left home. I feel empty and hurt” Milly 12yrs (quote from ChildLine 2007) Sexual Physical Emotional Continue Neglect
Children can experience problems outside the home as a result of parental alcohol or drug misuse these include; Children talked about being worried, frightened and confused by their parents’ alcohol and drug misuse Being bullied at school Problems with concentration at school due to lack of sleep or worries over their parents or siblings. Missing school to look after their parents or siblings “Mum goes out drinking. She doesn't come back until the morning. I am left to babysit my little brother and little sister. I can't sleep when Mum is out as I can hear noises downstairs.” Adrian, aged 14, (quote from ChildLine 2010) However, for some children, school can provide respite from their problems at home,
Parental mental ill health It is essential that staff working with adults consider the implications of a parent/carers mental health on children's welfare and parenting capacity. The majority of parents who suffer mental illness are able to care for and safeguard their children, however nationally 25% of children who are subject to Child Protection Conferences have a parent with mental health problems. What type of abuse is this? Select the correct answer to continue Sexual “Mum’s always miserable. She never asks me how I am. She just sits in front of the telly all day. I could be dead for all she cares” Wayne 13 years (quote from ChildLine 2007) Physical Emotional Continue Neglect
The following associated risks may justify a referral to social care for an assessment of the child’s needs and must be discussed with Team managers or the Trust Safeguarding Team: Suicidal thoughts involving a child Severe post natal illness Non compliance with treatment Delusional beliefs which include the child Children witnessing parental self harming behaviour This is also a wider issue which often indicates difficulty parents have with organising their own lives, they may neglect their own needs and in turn neglect the needs of their children. Unsupported and/or isolated mentally ill patients Conditions affecting parenting capacity -e.g. post natal depression
A report in 2009 by the National Patient Safety Agency reported that 30 murder convictions a year result from children killed by a parent or step parent. A third had a mental disorder Note: Where there is both parental mental illness and domestic violence and / or substance misuse, staff must make a referral to Social Care unless they can evidence why there is no risk to a child. Children with a parent with mental illness often receive little help in dealing with the effects of the parent’s illness. They often worry about their parents, blame themselves for the illness, fear they will ‘catch’ the illness and feel unsupported. These children need to be seen and heard.
Think Family Are the children safe How is the parent’s illness affecting the children Are there children in the family Do the children have someone to talk to Who is looking after them We cannot assume that someone else is talking with children and young people, and we should ensure that we communicate and work with other professionals where appropriate in order that children and young people can make sense of their parent’s illness and feel supported. Other professionals that can help with this includes: • Child & Adolescent Mental Health Service; • Health Visitors & School Nurses; • Children’s Social Services; • School Counsellors; • Voluntary Sector.
Previous history of safeguarding concerns Where a previous child/young person has been subject to a child protection plan (formerly known as the child protection register) Where a previous child/young person has been removed by the local authority (social care) Adults or young people known to be a Risk to a Child (formerly a Schedule 1 Offender) Child Factors • Age of the child, Children under one year are particularly vulnerable • Children and young people with any kind of disability are more vulnerable to abuse and neglect • Looked after children/young people (LAC) those in private or local authority foster care or children’s homes
Young People and Self Harm Self harm is a significant event and should form part of the chronology of events in the child’s life. Indicators may include: Self mutilation for example: cutting, hair pulling. Risk taking behaviour such as substance misuse Eating disorders such as bulimia Suicide threats, although serious suicidal intent is difficult to detect, 50% of completed suicides have a history of self harm but only 3% of children and young people that self harm end their lives
Professional response should include Taking the child/young person seriously Seeing the child Considering the possibility that self harm may have been triggered by any form of abuse or chronic neglect The impact on any siblings Multi disciplinary and/or agency assessment
Recognising factors that may Stop Children Telling It is important for practitioners to be aware of any factors that may prevent a child or young person from making a disclosure, the following is not an exhaustive list: May not recognise that what they are experiencing is abusive Direct threat to the child or young person not to ‘tell’ Lack of appropriate vocabulary due to age or disability Fear about reprisals, what may happen as a result of them ‘telling’ Feelings of guilt or shame, children often feel the abuse is somehow their fault Fear of not being believed, particularly where an abuser has told the child they won’t be believed Lack of opportunity to be heard Silence to protect others May have been made to feel ‘special’ by the abuser
Recognising factors that may Stop Adults Telling Not believing the child It is important for practitioners to be aware of any factors that may prevent adults from making a disclosure Uncertainty About procedure and consequences Child or young person’s attempt to bind them to secrecy A perception of not wanting to damage the relationship with a family Fear of being wrong Their own unresolved feelings Not believing that the abuser could have perpetrated the abuse, particularly if the abuser is someone close or someone they work with Always seek advice from your line manager or the Trust safeguarding children team if you are unsure about a disclosure
Confidentiality and Consent Giving consent is a process, not a one-off event. Staff cannot give assurance of confidentiality where there are concerns about a child as information may need to be shared in order to protect the child, and decisions relating to the child’s welfare can be taken in light of all relevant information. In the public interest: when gaining consent would place a child, young person or adult at risk of significant harm, crime prevention, fraud, public at risk if information not shared Consent to share information should always be sought where possible, except when; For children and young people: young people 16 – 17 years can consent to their own treatment. Court order: this cannot be argued As long as you can understand and weigh up the information you need to make a decision, you should be able to make it. - Department of Health, 2001 Young people under 16 where assessed as Fraser Competent can consent to treatment (child's age, intelligence / understanding, maturity, experience and the seriousness of the treatment) or as Gillick Competent can consent to contraceptive treatment (check and re-word if necessary)
What to do if you are concerned for the welfare of a child All staff have a legal duty to report any concerns they may have for the safety and welfare of a child. If you are concerned about a child or young person you must seek advice from the Safeguarding team and your line manager with a view to making a child protection referral. You MUST record all information and actions clearly with your name, designation, signature and date. However, You may need to ensure the child or young person’s immediate safety and access emergency assistance if necessary. You must then inform your Line Manager or the Trust Safeguarding Team. Outside normal working hours contact the Manager on call via switchboard. Referrals to children’s social care must be made within one day of identifying the concern and telephone contact must be followed up with a written referral within 48 hours. If the referrer has no contact from social care then they have a responsibility to follow up the outcome of the referral within 3 working days. If you are unable to contact your line manager or a member of the safeguarding team you should seek advice directly from children’s social care
Access to further information Staff should be aware of how to access the Trust Safeguarding Children Policy, Information sharing Guidance and Whistle blowing policy, including managing allegations made against staff who work with children. Staff must make sure they know how to access their local safeguarding children team contact details Information can be accessed via the Safeguarding site on the Trust Intranet which includes: National –A key document is Working together to safeguard children 2013, Local and Trust polices Safeguarding Team contact details and referral forms. Remember- Safeguarding children is everyone's responsibility, if something doesn’t seem right- seek advice from your line manager or Trust safeguarding children team.
For more information or to download these leaflets make a note of and go to the following website: http://www.nspcc.org.uk/inform/trainingandconsultancy/learningresources/coreinfo/coreinfo_wda54369.html
This now completes Safeguarding Children please continue to Safeguarding Adults



















