Download
1 / 24
240 likes | 317 Views
“Beyond Data Collection” or “What Should We Do Now We’ve Got The Results?”. Dr John Derry Medical Director Oxfordshire MAAG. Beyond data collection or “What should we do now we’ve got the results?”. Dr John Derry Medical Director Oxfordshire MAAG.

E N D
“Beyond Data Collection”or“What Should We Do Now We’ve Got The Results?” Dr John Derry Medical Director Oxfordshire MAAG
Beyond data collectionor“What should we do now we’ve got the results?” Dr John Derry Medical Director Oxfordshire MAAG
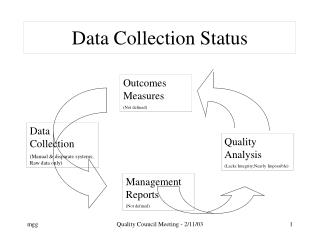
But what should we do? • See variation • What is significant? • Is it OK to be near average? • When should we act? • Where should we start? • How should we act?
Use of “SPC” • “Statistical Process Control” • Methods developed by Shewhart and Deming (1930s – 1990s) • Cornerstone of quality improvement • Two different kinds of variation can affect any process • Distinguish by statistical methods
“Statistical Process Control” • “First and foremost, a way of thinking with some tools attached” • “About the continual improvement of processes and outcomes” • “About getting the most from your processes” • Quotes from Don Wheeler in “Understanding Variation” SPC Press, 2000
Audience Participation! • How long does it normally take you to get to work? • Why does it vary? • So you already know about the two kinds of variation!
“Routine” “common causes” many factors, some “unknowable” “noise in the system” affects process most of the time part of the process variation is predictable “Exceptional” “special causes” “assignable” causes usually few, not many can usually be identified not part of the process intermittently apparent unpredictable variation Understanding variation
“Routine” don’t react to individual results look at the average and process limits improve the whole process if these not acceptable or continuously improve quality! “Exceptional” investigate each point outside the limits look for the special cause and do something about it almost always something to find opportunities to learn What to do about variation
Mistake 1 Act as if there is a special cause when there is only routine variation Might make things worse Wasted effort anyway Mistake 2 Fail to spot a special cause – assume there is just routine variation present Missed opportunity reduce variation improve quality learn something Two kinds of mistake
Control charts • Graphical method developed by Shewhart to help distinguish two kinds of variation • routine and exceptional • predictable and unpredictable • common and special cause • “Process behaviour charts”(Don Wheeler)
Plus 3 SDs Exceptional variation Average Minus 3 SDs Exceptional variation Anatomy of a control chart Control Chart of Clinical Audit Data 25 20 15 SqRt number with criterion Routine variation 10 5 0 0.00 20.00 40.00 60.00 80.00 100.00 SqRt number without criterion
Increasing difference Practices here are significantly different from average Practices here are significantly different from average Increasing difference How to interpret the chart Control Chart of Clinical Audit Data 25 20 15 Practices here cannot be distinguished from average SqRt number with criterion 10 5 0 0.00 20.00 40.00 60.00 80.00 100.00 SqRt number without criterion
“Double square-root chart” • Described recently by Mohammed et al (Lancet 2001; 357:463–467) • Originally developed by Fisher, Tukey & Mosteller in 1940s • Enable analysis of variation in “cross-sectional” data • Based on binomial probability distribution for calculating SD
Standardised CVD Prevalence Average = 4.6% +/- 3SD Range = 3.6-5.7% 25.00 20.00 434 413 416 407 15.00 409 420 SqRt number with CVD 424 10.00 406 405 417 5.00 429 0.00 0.00 20.00 40.00 60.00 80.00 100.00 SqRt number without CVD
10 293 9 200 8 257 57 115 206 7 146 6 311 43 PCT average 4.91 5 Rate per 100 Oxon average 4.72 80 4 78 145 54 3 2 4 1 0 71429 71417 71406 71420 71430 71418 71428 71412 71410 71415 71422 71414 71423 71427 71408 71411 71409 71413 71407 71424 71416 71405 71434 Practices CHD Audit Resultsage & sex standardised prevalence of CVD
Average = 76% +/- 3SD Range = 61-84% 20.00 15.00 434 416 412 SqRt number with BP record 10.00 430 5.00 417 411 422 0.00 0.00 2.00 4.00 6.00 8.00 10.00 12.00 SqRt number without BP record BP recorded
14 80 100 200 85 173 90 257 235 80 173 70 293 43 60 28 54 50 Percentages 40 30 20 BP not in target values <150sys <90 dia BP in target values <150 sys <90 dia 10 0 71417 71434 71414 71423 71429 71413 71427 71408 71420 71410 71416 71430 71418 71411 71412 71428 71406 71405 71424 71409 71407 71415 71422 Practices CHD Audit Resultsblood pressure recording & control
Control charts for clinical audit • To answer the question • “What do we do now we’ve got the results?” • To identify where to target efforts • To know when to act • To know what kind of action to take