Download
1 / 18
190 likes | 357 Views
Science R & D Innovation. Knowledge Ware Trust 2002 ‘The Missing Billion’ Speech from the Throne 2005 ‘Science critical to driving New Zealand Economy’ Prime Minister John Key 2009 ‘Science and innovation will be at the centre of my government’

E N D
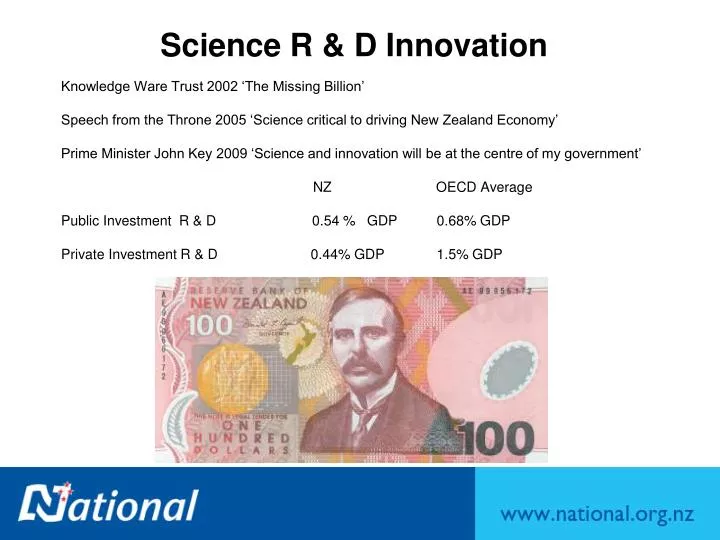
Science R & D Innovation Knowledge Ware Trust 2002 ‘The Missing Billion’ Speech from the Throne 2005 ‘Science critical to driving New Zealand Economy’ Prime Minister John Key 2009 ‘Science and innovation will be at the centre of my government’ NZ OECD Average Public Investment R & D 0.54 % GDP 0.68% GDP Private Investment R & D 0.44% GDP 1.5% GDP
Improving NZ Environment To Support Innovation Through Clinical Trials “Prof. Shaun Holt ‘our ethics system is now so unwiedly, its unethical” – NZ Herald March 2009 Prof. Tim Dare “Health Ethics Committee up with world standards” – NZ Herald 16 March 2009 Holt “Problems with Ethics Committee – lack of expertise, overly bureaucratic, complicated application forms, slow…” Rudd Government Taskforce 2009 “To make Australia the best place in the world to carry out clinical trials. Report due April 2010?
Improving NZ’s Environment to Support Innovation Through Clinical Trials New Zealand: Phase I-IV trials worth $12 - $20 million Australia: Phase I-IV trials worth $450 million Terms of Reference Co-ordinated, nationwide approaches to clinical trials Streamline ethics approval systems National patient referral networks Removal unnecessary barriers How to benefit the NZ innovation system, health system, & economy Rationale – Multibillion Dollar Industry Good for patients, standards, health systems, scientists Good to stimulate biopharmaceutical, functional food and medical device industry in New Zealand – good for the economy.
London 1921 ? The Missed Opportunity Glaxo Smith Kline 2007 Turnover $66 billion dollars per year R&D spend $10 billion New Zealand dollars Bunnythorpe 1900 Glaxo Foot Rot Vacinne
Singapore – The Biopolis of Asia “You can’t buy Wrigley’s Spearmint gum in Singapore. But human embryonic stem cells? That’s a different matter…”
Professor Shaun Holt, Geoffrey Horne Should have smaller committees – 7 rather than 12 No need to have Justice of the Peace sign off No need to consult Maori every study No need for locality assessment forms Simple 1-2 page applications system for simple studies On line applications – forms reduced by 50% Committee lead reviewer for each study should email researcher to clarify any potential ethical problems before the meeting Letters should be emails to researcher within 3 days of meeting
Recommendations for Improvement – Chairs/Health and Disability Ethics Committee Introduce an on-line application and approval process. Improve application form to remove repetition and ambiguity. Provide a central clearing house to allow researchers to have their application reviewed by their regional committee, or by the committee meeting next if they want their application fast tracked. Ensure that there is at least one Ethics Committee meeting somewhere in the country every week, except for the Christmas/New Year period. Retain regional committees to facilitate attendance by researchers. Where this is happening applications are approved more quickly and good working relationships have developed. Establish a dedicated committee for sponsored clinical trials for which a fee will be charged.
Recommendation for Improvement cont’d Consider reducing membership to 10 but retain 50% balance lay/non-lay membership. Public confidence and quality are essential and a comprehensive mix of skills supports thorough analysis and sound outcomes. A pool of experts could be established whose advice could be drawn upon as needed. Terms of reference for expedited review be considered with a view to widening scope where appropriate. Establish review turnover times as a monitored performance measure. Enable researchers to instigate minor amendments and inform committees. Update the Operational Standard to cover areas where there is inconsistency and provide appropriate and timely training for all committee members.
Medical Technology Association of NZ (MTANZ) Medical technology industry Annual turnover $1.3 billion 2008/2009 Export income $333 million 200707/2008 Employs ≥ 6000 people Research investment $56.6 million 2007/2008 Recommendations A better understanding of the differences between medical technologies & pharmaceutical and the data required to support the respective products through development. A centralised ethics process in order to speed up the approval process. Ethics committee to engage with applicant in meaningful dialogue that is transparent with feedback. Ethics committee to have a formalised monitoring programme with agreed time lines for applicants.
Medical Technology Association of NZ (MTANZ) cont’d A mutually agreeable standardise Indemnity Agreement (IA) & Clinical Trial Agreement (CTA) should be developed. Better access to clinicians & better support from the public hospitals for local medical technology industry. Government support (financial support through grants, in-kind support, tax concessions…) for all phases of clinical research – from new technology innovation, to proof of concept trials, to multicentre global studies. Mutual Recognition Arrangement (MRA) between Australia & New Zealand for the ethics process.
NZ BIO Submission NZ develop a notification system similar to Australia – recommends Clinical Trial Notification (CTN)/exemption (CTX) system. That operating guidelines to Medsafe, SCOTT & GTAC, expressly encourage meeting with sponsors before an application is submitted & after it has been reviewed. That overseas experts should be considered to expand the talent pool for SCOTT. That the process for trials involving functional foods be separated from the therapeutic clinical trial process & simplified to remove non-relevant requirements such as toxicology studies on food with a long history of safe consumption.
Realising NZ’s Potentialminimise systemic weaknesses (Roche) Speed to start up Improvements in Ethical review Ethics approval in parallel timeframe to SCOTT Invest in electronic information management (online submissions) Networked decision making (committee need not “sit”) Increased capacity & capability Regionalisation of Research Development Offices Decreased duplication amongst DHBs, ethics committees & SCOTT Nationally consistent infrastructure & culture to support clinical trials Establish & collect performance metrics Public education & participation Cohesive policy development, process improvements Privacy Act Uniform focus on professional development & training Accredited training & career pathways Optimal resource management & cost containment Electronic patient database & patient referral networks Patient identification & recruitment NHB IT Board
Innovation in NZ Health Delivery ResearchWeakly distribute policy & investment (Roche) “Igniting Potential” NZ’s Science and Innovation pathway strategy Health & Society research sector outcomes 1/6th of focus No specific policy directions from this sector MOH does not have a research strategy Research specifically excluded from DHB operational funds DHB Staff involvement in research not regarded as legitimate activity Recognition Reimbursement Core job responsibility NZ Government funding per capita for health research 1/3 Australia, 1/5 UK, 1/10 USA. Responsibility for policy & funding of health delivery research distributed across multiple agencies (e.g. FRST, MORST, HRC, MoH) Contrast UK NIHR, Australia NHMRC
Number of Industry Funded Studies Listed in ClinicalTrials.gov (Roche)
South KoreaGovernment Investment Critical Success Factor(Roche) Regional Clinical Trial Centres (CTC) programme supported by the MOHW (Ministry Health & Welfare) 14 centres of excellence established USD – 4 million per centre & matching fund from each institution “One of the key factors in boosting the growth of clinical trials in Korea was the government recognition of their key role in driving the development of the biotech & pharmaceutical industries, as a truly knowledge-based activity”. Ref: Prof San_Goo Shin. President of KoNECT December 2008 interview, KoNECT website News Board http://www.konect.or.kr/eng/
Improving NZ’s Environment to Support Innovation through Clinical Trials Unanimous Robustness of ethical evaluation must remain Room for significant efficiencies in process Task for Health Select Committee Analyse the 71 submissions, advisors from Ministry of Health and MORST along with independent advisor David Clarke, Make recommendations, to make NZ environment, best practice, (best in the world) to carry out clinical trials.