Download
1 / 14

E N D
Case • Samantha is a 15 year old girl attending the clinic, seeking your help. She reported having had a one-night-stand sex with her ex-boyfriend just 4 days ago. Yesterday, she received a message from him to inform her that he is being treated for STI. Her friend have advised that she sees her doctor because she might have caught something.
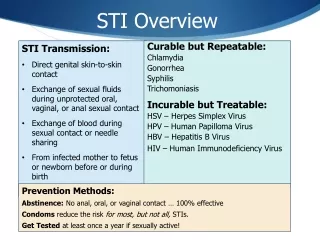
HISTORY TAKING • Basic rules: • Introduction- • creating rapport • confidentiality assurance. • Avoid assumptions • Avoid being embarrassed yourself • Be non-judgemental • Use of condoms does not confer absolute protection. • Be clear that sex includes oral and rectal routes.
WHAT TO ASK ABOUT • -menstrual (?pregnancy, idea of what her normal is) • -sexual (number/ type of partners, use of barrier methods, type of sexual practices) • -contraceptive: methods and compliance • -social history: under 16s: family and care/ alcohol and drug/ child abuse and neglect/ financial difficulty and prostitution.
History of symptoms of STI. • -vaginal discharge • -IMB/ PCB • - lower abd / pelvic pain/ dyspareunia • - menstrual changes; flow, duration, new dysmenorrhoea etc • - genital rash/ ulcer • -general well being
FRASER GUIDELINES • The Fraser guidelines are a set of criteria which must be fulfilled when contraceptive services are provided to people less than 16 years of age without their parent's knowledge or permission: • The young person UNDERSTANDS the advice given to her by the health professional. • The young person cannot be persuaded to inform PARENTS, or to allow the health professional to inform them (CONFIDENTIALITY). • It is likely that the young person will continue to have SEXUAL intercourse, with or without the use of contraception. • The young person's physical or mental health may SUFFER as a result of withholding contraceptive advice or treatment. • It is in the best INTEREST of the young person for the clinician to provide contraceptive advice or treatment, or both, without parental consent.
Consent issue • Assess a young person's competence to consent to treatment by her ability: • To understand the information provided and • To weigh up the risks and benefits and • To express her own wishes. • If a young person is determined to be competent, this should be documented in the case notes. If determined incompetent, discuss involving an adult she trusts, preferably parents/ other family/ carer/ social services.
The mnemonic UPSIC (UnProtected Sexual InterCourse) can help to remember all these points: • Understands • Parents • Sex/Suffer • Interests • Confidentiality; Coercion an issue? • [Guillebaud, 2007]
Risk assessment 1 • Pregnancy and pregnancy test. • consider emergency contraception • (?oral or IUCD) • - risk of STI and IUCD insertion. • - oral contraception and limitations • Consider long term contraception, offer Long acting contraceptive methods.
Risk assessment 2 • STI: local prevalence, age, sexual activity and age at onset, frequency or change or multiple sexual partners, alcohol and drug use, unprotected sexual activity and contraception, visit to or coming from HIV prevalence area.
Who should you treat? • If any symptoms/ signs suggestive of STI • - treat a/c to suspicion • - make good use of available limited tests e.g swabs and chlamydia kits • - Refer to GUM; discuss necessity/ confidentiality and briefly what likely to happen there/ give contact. • (risk of not attending the GUM, be sure you have right contact details)
If no symptoms or sign, • Assess patient’s enthusiasm to attend GUM clinic, • If low, maximise simple tests available e.g clamydia kit and GUM advice • If high, GUM advice.
Contact tracing • Important to raise it with patient: necessity and confidentiality. • Who needs contacted • How ? – self contacting (direct and indirectly) • - ? Through health professional
Useful references. • http://www.rcgp.org.uk/PDF/clinspec_STI_in_primary_care • http://www.nhs.uk/Conditions/Sexually-transmitted-infections/Pages/Introduction.aspx • http://www.ffprhc.org.uk/admin/uploads/326_VaginalDischargeGuidance.pdf