Download

1 / 69
760 likes | 1.7k Views
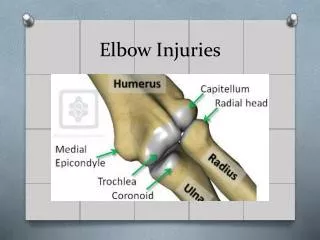
Elbow injuries and the throwing athlete. Michael J. Kissenberth MD Orthopaedic Surgery, Sports Medicine SHCC, Greenville Hospital System. First Question. What sport do you play?. Most sport related elbow injuries are caused by repetitive microtrauma….

E N D
Elbow injuries and the throwing athlete Michael J. Kissenberth MD Orthopaedic Surgery, Sports Medicine SHCC, Greenville Hospital System
First Question What sport do you play?
Most sport related elbow injuries are caused by repetitive microtrauma…
And the underlying pathology is directly related to the biomechanicsof the sport.
Second Question • Where does it hurt? • Anterior • Medial • Posteromedial • Posterior • Lateral
Third Question 3. When does it hurt?
1st Critical Instant Andrews
2nd Critical Instant Andrews
Restraint to Valgus Torqueat 90 Degrees FlexionUCL 54%RC Articulation 33%Capsule 10%
Medial Tension ME injury Sigmoid rim fx FP mass injury UCL lesions UN neuritis Lateral Compression RC joint injury Synovitis Effects of Valgus Torque
History • Medial Pain • Late Cocking, Early Acceleration • Recurrent Symptoms • Pop on Single Throw • Swelling, Stiffness • Lost Performance!!!
Previous Treatment • Lost Playing Time • Rehabilitation • Injections • Diagnostic Studies • Surgery (VEO)
Examination • Medial Swelling • Motion Loss • UCL Tender • Valgus Stress Painful • Valgus Laxity • Associated Findings
Kids • ME Apophysitis • ME Fragmentation • ME Avulsion
ME Apophysitis With Fragmentation Without Fragmentation
14 y/o BB Player No prior symptoms “Pop!”
FP Muscles - UCL FPM The flexor pronator muscles provide varus torque UCL ME Ulna Flesig AJSM 95, Werner JOPST 93
Pronator Muscle Tear 27 y/o RHP Conjoined Tendon
Severe FPM / ME Think UCL Injury!!!
Rarely inject FPM Deep Massage Modalities Rehabilitation Repair ME
Treatment Relative / Active Rest Ice, NSAID Local Modalities Prevent Atrophy Treat Associated Conditions NO Steroid Injections!!!
Treatment Strengthen FCU, FDS Trunk, Scapula, Cuff Stab. PNF, Plyometrics Sport Specific Exercise Review Throwing Mechanics Interval Throwing Program
UCL Complex • Anterior Bundle • Strongest portion • Insertion on sublime tubercle • 18 mm posterior to coronoid tip • Origin is inferior and posterior to rotation axis • Tighter in flexion
Milking Maneuver UCL Tests Static Valgus Stress
Moving VST O’Driscoll Likely best test
Avulsion Fracture Sublime Tubercle Glajchen AJR 1998
Rehabilitation Initial Immobilization Relieve PainResolve Arm SwellingRecover Range of MotionPrevent Muscle Atrophy Restore Aerobic ConditionMaintain/develop core stability
Toss 4 - 5 MonthsMound 6 - 8 MonthsGame 11 - 12 Months Prevent Shoulder Injury
Ulnar Nerve Injury Fibrosis Compression Tension UN subluxation Elbow valgus laxity
Non-operative Care • Night Splint • NSAIDs • Oral Steroids • Activity Modification • Desensitization / Soft tissue release
Decompression 4 3 2 1 ME
Fascia Sling ME
Lateral CompressionInjuries Rad-Cap arthrosis Stress fracture OCD Lateral synovium
Kids – Lateral Elbow • Panner’s Disease • <10 yo, self limited • OCD Capitellum • Progressive!!!
Panner’s Disease • OCD capitellum • 5-10yo • Self limited • Tx conservatively • Rest, ice, nsaids • Gradual RTP. Must be able to throw without sx
Posterior blood supply peds lateral elbow Repetitive injury to epiphysis may alter blood flow = osteochondrosis
Osteochondritis Dissecans • Age 9 - 16 Years Old • Progressive • Remove loose bodies