Download
1 / 73
861 likes | 1.33k Views
Cardiac tumors. Dr Shreetal Rajan Nair Senior Resident, Department of Cardiology, Calicut Medical College. History . 1559 : Columbus , a noted pathologist – first to report 1934 : first report of a primary sarcoma of the heart diagnosed in a living patient by Barnes

E N D
Cardiac tumors Dr ShreetalRajan Nair Senior Resident, Department of Cardiology, Calicut Medical College
History • 1559 : Columbus , a noted pathologist – first to report • 1934 : first report of a primary sarcoma of the heart diagnosed in a living patient by Barnes • 1942 : surgical resection of intrapericardialteratoma by Beck • 1951 : The first successful excision of a cardiac tumor performed by Maurer • 1952 : Goldberg diegnosedintracavitarymyxoma by angiocardiography • 1968 : Shattenberg used echo to diagnose cardiac tumors
Classification Primary benign (75%) malignant (25%) Myxoma – 50% Rhabdomyoma – 20% Fibroma Papillary fibroelastoma Lipoma Angiosarcoma Rhabdomyosarcoma Leiomyosarcoma Lymphomas secondary Breast lungs
Incidence • All age groups - 0.002% to 0.03% • Pediatric - 0.027% to 0.08% • Adults - upto 0.02% • By comparison, metastatic involvement is 20 times more common
Incidence of benign tumors Shapiro LM. Cardiac tumours: diagnosis and management. Heart 2001; 85: 218 - 22.
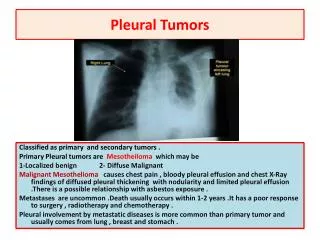
Tumors of the heart - • Constitutional or systemic • Embolic • Cardiac • Phenomena secondary to metastatic diseases. Specific signs and symptoms generally are determined by the location of the tumor, size, friability , mobilityin the heart and depends least on the histopathology
Tumors of the heart- clinical presentations • Primary tumors most commonly involve the endocardium, followed by myocardium and then epicardium • Metastatic involvement of heart is reverse that of primary tumors • Endocardium- obstruction to flow of blood through heart • Myocardium - rhythm abnormalities • Epicardium – pericardial effusion, cardiac tamponade
Approach to a cardiac tumor Differential diagnosis • PUO • IE/CONNECTIVE TISSUE DISEASES • VALVULAR LESIONS • CCF • CONDUCTION ABNORMALITIES • EMBOLISM • SYNCOPE • PERICARDIAL EFFUSION
Diagnostic evaluation • Confirm the diagnosis • locate the lesion within the heart • Whether benign or malignant
Echocardiography • Simple, noninvasive technique for initial evaluation. • Images myocardium and the cardiac chambers Identify the presence of a mass and its mobility. • Information about any obstruction to the circulation & whether the tumor could be a source of emboli
Echocardiography - TEE vs TTE Transthoracic echocardiography – the initial diagnostic tool Transesophageal echocardiography (TEE)- more informative. This is due to the proximity of the esophagus to the heart, the lack of intervening lung and bone, and the ability to use high-frequency imaging transducers that afford superior spatial resolution
CARDIAC MRI VS CT • Both provide noninvasive, high resolution images of the heart, but MRI generally is preferred. • cMRI -detailed anatomic images T1- and T2-weighted sequences help to identify the chemical microenvironment within a tumor • CT -useful when calcification is present and MRI is not available or is contraindicated.
CORONARY ANGIOGRAPHY • Mapping the blood supply of tumors arising from the epicardial surfaces • vital to the success of excising such tumors. • Significant involvement of coronary arteries - resection and grafting of such arteries
Role of Transvenous biopsy • Limited data are available on the risks and benefits • considered reasonable if potential benefits outweigh risks and there is diagnostic dilemma
Benign tumors • Around 75 percent of primary cardiac tumors are benign • In adults, most common- myxomas (50%) • Other common benign lesions- papillary fibroelastomas and lipomas. • In children, the most common- rhabdomyomas and fibromas
Myxomas • Most common primary cardiac neoplasm. • Histology- scattered cells within a mucopolysaccharidestroma which originate from multipotentmesenchymal cells capable of neural and endothelial differentiation . Hallmark histological feature is myxoma (lepidic) cell • Produce VEGF-induction of angiogenesis and the early stages of tumor growth & IL 6 -responsible for the constitutional features.
Myxomas • Typically pedunculated and gelatinous in consistency; smooth, villous, or friable. • Calcification , necrosis and cystic changes seen • Mostly (90%) solitary • About 35 % of are friable or villous, these tend to present with emboli. • Larger tumors -smooth surface and associated with cardiovascular symptoms.
Myxomas • The cardiovascular manifestations depend upon the anatomic location of the tumor. • Mostly seen in females • 40-60 years of age • 80% -originate in the left atrium, most of the remainder is found in the right atrium • constitutional symptoms (eg, weight loss, fever) and laboratory abnormalities
Syndrome Myxoma Characteristics Syndromic associations • Younger than 40 years • Biatrial ,ventricular , valves • all first degree relatives should be screened • Recurrent – 30% • No gender predilection • LAMB (lentigines, atrialmyxomas,mucocutaneousmyxomas, and blue nevi), • NAME(nevi, atrialmyxomas, myxoidneurofibroma, and ephelides • Carney syndrome (atrial, cutaneous and mammary myxomas, lentigines, blue nevi, endocrine disorders and testicular tumours)
Myxoma Carney syndrome Histological features Mutations in : • PRKAR1A (protein kinase A regulatory subunit 1A ) • MYH8 - myosin isoform • PAS • Vimentin • S100 and NSE - POSITIVITY
Treatment • Prompt resection-due to the risk of embolization or cardiovascular complications, including sudden death • Result of surgical resection is good ( <5% mortality) • Cardiac autotransplantation
Papillary fibroelastomas • Second most common primary cardiac tumor in adults • Their appearance is compared to pom-pom or sea anemones
Clinical features • Symptoms -caused by embolization of the tumor/thrombus. • most common clinical presentation- stroke /TIA. • Commonly attached to the aortic valve • 30%- incidentally diagnosed by echocardiography, at cardiac surgery, or at autopsy
TREATMENT • SURGERY – 1. patients who have had embolic events or complications directly related to tumor mobility (eg, coronary ostial occlusion) 2.Those with highly mobile or large (≥1 cm) tumors • Recurrence not reported
Lipomas • Lipomas &fibrolipomas - characterized by a predominance of benign fatty cells. • About half of these tumors occur in the subendocardialregion.Others in the myocardial and subepicardial regions • They may also occur on valves
Lipomas • Symptoms- generally related to local tissue encroachment (arrhythmias, conduction block, sudden death) valvular tumors – insufficiency & symptoms of heart failure • Diagnosis - echocardiography and the distinctive fat pattern on MRI. • Require resection.
Lipomatous hypertrophy of the interatrial septum • Exaggerated growth of normal fat existing within the septum and is not a true tumor. • Developmental disorder caused by expansion of adipose tissue trapped in the interatrial septum during embryogenesis • The septal hypertrophy may be as much as 2 cm in thickness and is seen primarily in older patients and in those who are obese
Lipomatous hypertrophy of the interatrial septum • Associated with the presence of CAD in proportion to the degree of atrial septal thickness • Indistinguishable from lipoma except that the former occurs in the atrial septum with a typical distribution (generally sparing the fossaovalis). • In the absence of symptoms of atrial arrhythmias, heart block or rare vena caval obstruction, they do not require resection
Pericardial lipomas • Incidental finding and clinically insignificant. • Rarely assumes gigantic proportions and its appearance on a chest radiograph may be mistaken for a huge pericardial effusion or massive cardiomegaly • Benign pericardial lipomas can infiltrate the myocardium. If the ventricular septum is invaded, communication between the pericardial space and the right ventricular cavity may result.
Rhabdomyomas • Develop almost exclusively in children, mostly <1 year of age • 80 to 90% are associated with tuberous sclerosis • Usually found in the ventricular walls/AV valves. • Most regress spontaneously • Resection is usually not required unless symptomatic • Symptoms –due to obstruction of blood flow through the heart or consist of rhythm disturbances • Present with features of preexcitation on the ECG
Rhabdomyositis • A rare form of cardiomyopathy in infants • Tumor nodules are not grossly apparent • Microscopically, the cardiac muscle fibers and conduction system are diffusely involved with rhabdomyomatoushistologic changes • Recurrent atrial tachycardia and sudden death from intractable ventricular tachycardia
Why rhabdomyomas regress? • High expression of ubiquitin which starts expressing from 32 week onwards • Absent mitotic activity • Ubiquitin is responsible for the degradation of rhabdomyoma cells and hence tumor regression • Characteristic spider cells are formed in the process.
Fibromas • Second most common pediatric cardiac tumor and can also occur in adults • Histologically similar to fibromas arising elsewhere in the body. • Usually arise in the ventricular muscle and may become quite large. • Do not regress spontaneously. • Arise approximately 5 times more frequently in the LV than RV
Fibromas • Most common symptom, due to obstruction of blood flow or interference with valvular function. • Myocardial dysfunction and conduction disturbances • Echocardiography, supplemented with CT/MRI confirms the diagnosis. • Symptomatic tumors should be resected. Complete resection of very large tumors may require cardiac transplantation.
Teratomas • Arise within the pericardium, but do not originate from cardiac structures • Although generally benign,can have serious mechanical consequences by causing tamponade or through direct pressure on the heart. • Risk of death in-utero or immediately after birth
Teratomas • Treatment therefore requires either fetal tumor excision, or caesarean section and immediate operation on the newborn • Have a single blood supply and are not invasive, properly timed tumor surgery is straightforward and successful
Purkinje cell tumors/hamartomas • Consist of small, flat sheets of cells most frequently located in the left ventricle, and on the endocardial and epicardial surfaces • Undetectable by echocardiographic or radiologic techniques. • Tumors of young children and present with incessant ventricular tachycardia • ECGs often demonstrate a bundle branch pattern (right bundle branch block when the tumor is in the left ventricle). Electrophysiologic studies can localize the tumors, facilitating surgical excision.
Paragangliomas • Neuroendocrine tumors that can be hormonally active or inactive. • In tumors not producing catecholamines, symptoms are due to cardiac compression or tamponade. • In contrast, cardiac paragangliomas that are hormonally active primarily produce norepinephrine and may cause systemic symptoms (eg, headache, sweating, tachycardia, hypertension) • Hormonally inactive tumors are more frequent in the pericardium
Paragangliomas • May be localized with echocardiography. • Extremely vascular • Coronary angiography -to plan the operative resection
Paragangliomas • Paragangliomas (benign/malignant) within the pericardium parasitize the cardiac blood supply and hence are very difficult to excise • All intrapericardialparagangliomas require resection • Cardiopulmonary bypass and even circulatory arrest may be required due to the high degree of vascularity, or to moderate the extreme hypertension possible from tumor manipulation or hormonally active tumors • If complete resection is not possible, cardiac transplantation may be required