Download
1 / 41
450 likes | 827 Views
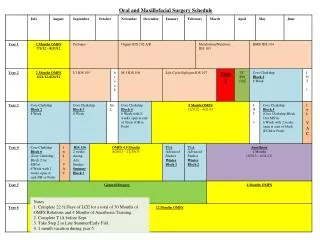
Anesthetic management of maxillofacial surgery. By: Alaa Samir El Kateb Lecturer of anesthesia and intensive care Ain Shams university. Objectives:. - Preoperative airway assessment. - Learn how to perform awake intubation. - How to draw a fluid chart.

E N D
Anesthetic management of maxillofacial surgery By: Alaa Samir El Kateb Lecturer of anesthesia and intensive care Ain Shams university
Objectives: • - Preoperative airway assessment. • - Learn how to perform awake intubation. • - How to draw a fluid chart. • - What is massive blood transfusion and its • complications. • - Know complications and prevention of • hypothermia.
Le fort classification Transverse crossing floor of nose, separating of the palate from the maxilla. Fracture of maxilla, where body of the maxilla is separated from the facial skeleton (pyramidal in shape) The entire maxilla and one or more facial bones are completely separated from the craniofacial skelton
Anesthetic consideration • Airway management (intubation & • extubation) • Blood loss • Hypothermia • Eye protection
Airway assessment • 1- HISTORY: • *Rheumatoid - *Morbid obese • *Submandibular abscess *Retropharyngeal abscess • *Neoplasm, Radiation, *Scleroderma • *Previous tracheostomy *Prolonged intubation • *Bleeding lesions *Syndroms e.g. Down • *Mandibular, maxillary &/or cervical spine fractures • *History of difficult intubation
Cont. Preoperative airway evaluation • 2- PHYSICAL EXAMINATION: • Thick , short & muscular neck • Receding or hypoplastic mandible • Edentulous, prominent incisors • High arched palate, large tongue • Presence of ear or hand deformities
Cont. Preoperative airway evaluation • Hyomental distance: 2 fingers • Thyromental distance: 6.5 cm • Mouth opening: (TMJ) 3-4 cm • Neck Movement: 35 degree flexion at • lower cervical and 80 degree • extension at atlanto-occipital
Cont. Preoperative airway evaluation • Mallampati’s : sitting, vocalizing, tongue protruded
- Cormack and Lehane scale The vocal cords visible The vocal cords partially visible (posterior commissure) Epiglottis Not seen Only epiglottis
Innervation of nasal, oropharyngeal & laryngeal cavities • Nasal/Nasopharyngeal Cavity –Trigeminal Nerve (CN V) • Oropharynx- • Glossopharyngeal Nerve (CN IX) • Larynx & Trachea – • Branches of the Vagus Nerve (CN X)
Anesthesia of the Nasal Mucosa and Nasopharynx(Sphenopalatine ganglion and ethmoid nerve) • - Lidocaine + epinephrine or • lidocaine + phenylephrine • - Long cotton-tipped applicators: • 1st: 45 degree to the hard palate • 2nd: parallel to the dorsal surface of the nose • - Left in place for 5 minutes • - Should be done bilaterally
II. Anesthesia of the mouth, oropharynxand base of tongue (Glossopharyngeal & superior laryngeal nerves) • - Lidocaine gel on tongue blade and • patient "sucks“. Peak on set 15 min. • OR Lidocaine can be placed in a • nebulizer for 5-7 min • OR The tongue and posterior pharynx • are sprayed with the atomizer.
III. Anesthesia of the hypopharynx, larynx and trachea Transtracheal block (RLN)
After anesthetizing the airway you may use: • Direct laryngoscopy • Blind intubation • Retrograde intubation • Fiberoptic intubation • PLEASE • Maintain spontaneous breathing
combitube ctrach COPA ILMA
LMA_supreme2 glidescope video assessted AIRtraq
Nasal intubation • - Vasoconstrictor 30-45 minutes earlier. • - Insert ETT parallel to hard palate. • - Bevel is medial (turbinates are lateral) • - During blind nasal: • _ Introduce the ETT during inspiration • _ You may use capnography
Fiberoptic bronchoscopy • - May turn to be an emergency situation. • - If to be used, use it as the first choice. • - Pull the tongue forward, jaw thrust. • - Put the patient in sitting position. • - Keep the midline against hard palate. • - You may dim room light and use it as • illuminating stylet.
Safe extubation • “air leak test” is done to evaluate whether or not the patient is capable of breathing spontaneously • You may use a hollow introducer or a tube-exchanger, bronchoscope or NGT
- Wide pore canula / central venous access Fluid therapy Deficit Maintenance Losses • Ryle • UOP • Bleeding • 3rd space • loss Hourly maintenance * fasting hours • 4 cc/Kg for 1st 10 weight • 2 cc/Kg for 2nd 10 weight • 1 cc/Kg for remaining • weight
Gross’s simplified formula • Allowable blood loss = • [(Starting Hct – target Hct) / Starting Hct] • X Estimated blood volume. • Estimated blood volume • Adults: 65-75 cc/kg • Infants: 80 cc/kg • Neonates: 85 cc/kg • Newborn: 100-120 cc/Kg • Amount to be transfuse (ml)= • [Target haemaglobin – Current haemaglobin] • X 4 X weight (kg)
Massive blood transfusion • American Association of Blood Banks definition: • 10 units of blood in 24 hrs • or 5 units of blood in 4 hrs
Complications of massive blood transfusion • 1- Coagulopathy: At least 1.5 times blood • volume to become a clinical problem. • 2- Hypothermia. • 3- Citrate toxicity: > unit/5 min • 4- Hyperkalemia
Complications of hypothermia: • 1- Arrhythmia: PVC (<30°C) – VF (<28°C) • 2- ↓ O2 delivery to tissues: O2 dissociation • curve, VC, ↑ blood viscosity. • 3- ↓ GFR and UOP stops at 20°C • 4- ↑ blood viscosity, ↑ rouleaux formation, • coagulopathy (depressed clotting • mechanism and platelets function). • 5- Metabolic acidosis. • 6- Post-operative shivering.
How to prevent? • - ↑ ambient air temperature. • - Humidify inspired air • - Warm mattress • - Plastic or cotton wraps • - Warm fluids
Any questions?? • Thank you