Download
1 / 52
520 likes | 625 Views
depth of anaesthesia monitoring after subarachnoid haemorrhage... comfortably numb?. douglas duncan western general hospital edinburgh. will cover 1. why we thought it would be useful 2. which patients we looked at 3. what we did 4.how we analysed the results, PK, sensitivities.

E N D
depth of anaesthesia monitoring after subarachnoid haemorrhage... comfortably numb? douglas duncan western general hospital edinburgh
will cover 1. why we thought it would be useful 2. which patients we looked at 3. what we did 4.how we analysed the results, PK, sensitivities. 5. summary.
how did this happen? Melbourne 2002 Royal Melbourne Hospital B-Aware Trial return to UK
why did we think this would be useful GDC (Guglielmi Detachable Coils ) Anaesthesia - issues • The patient must not move under any circumstances. TIVA and paralysed (at WGH), access to patient limited. • 2. Many of these patients are of decreased conscious level prior to any anaesthetic being given. Underdose/Overdose. • 3. The degree of surgical stimulation is probably very low. • 4. Catastrophic intracerebral events – cerebroprotection. • 5. We DO NOT think awareness is an issue.
Microcatheter is placed through the parent blood vessel into the lumen of the anuerysm. GDC microcoils are placed through the microcatheter into the aneurysm lumen. The coil is detached (fuse) from the pusher wire which is then removed. Additional coils are then placed sequentially until the aneurysm will not accept any more coils
SAH within days Vasospasm – conscious level +/- SAH recovered/good neuro function GDC Anaesthesia – patients • 2 patient groups • elective. • emergency.
Methods and Materials • MREC and LREC approval. • Patients undergoing ‘coiling’ recruited. • All had recent subarachnoid haemorrhage. • Total 38 patients. • Standard monitoring. • ECG, Pulse, IBP, SpO2. • Datex-Ohmeda S/5 Monitoring. • Propofol, remifentanil, atracurium anaesthetic. • Entropy and Bispectral index monitoring. • Entropy M Module, BIS XP • Indices recorded /5seconds • Laptop PC • Datex-Ohmeda S/5 Collect software • All drug dosing and changes to infusion recorded manually.
Average “bleed-coil” time = 4.95 days (min 1, max 22) Patient Demographics WFNS score 1. GCS 15, No motor deficit or aphasia. 2. GCS 13-14, No motor deficit or aphasia. 3. GCS 13-14, Any motor deficit or aphasia. 4. GCS 7-12, With or without deficit. 5. GCS 3-6, With or without deficit
anaesthetist – blind to BIS/Entropy indices why? don’t know the numbers mean anything.
When did we take the data.. .....continuously but looking particularly at..... 1.Presedation = 15secs data immediately prior to first sedative drug 2. LOC = 15 secs data, starting at no verbal response, no eyelash reflex 3. Intubation = 15 secs data starting 60 prior to ET tube passing through vocal cords 4. Stable = 15 secs data immediately prior to femoral catheter puncture 5. Eyelash return = 15 secs data after return of eyelash reflex only 6. Extubation = 15 secs data after patient extubated. = 6 clinically distinct depths + approx 75 hours data
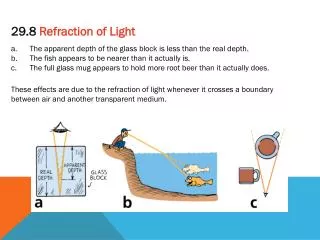
Measuring the Performance of Anesthetic Depth Indicators. Anesthesiology. 84(1):38-51, January 1996. Smith, Warren D. PhD; Dutton, Robert C. MD; Smith, N. Ty MD one of the properties of an ideal monitor includes; 1. Monotonicity – increasing clinically observed depth must always agree with increasing indicated depth. PK describes this
PK Measure of “degree of association” is decreasing BIS/ENTROPY number associated with increasing clinical depth – ie is there concordance? number between 0 and 1 1 indicates ideal concordance 0 indicates ideal discordance 0.5 equals a chance concordance.
100 60 40 20 PK=1 100 100 70 100 PK 0.58 original graphic Dutton, Smith, 1996
PK for lightening PK for deepening
PK verbal BIS 0.89 – 0.91 RE 0.83 – 0.88 SE 0.81 – 0.86 Vanluchene et al BJA Nov 2004
BIS return eyelash pre-sedation LOC intubation stable extubation
RE return eyelash pre-sedation LOC intubation stable extubation
ROC curves reminder (Receiver Operative Characteristics) 1.0 sensitivity 1.0 1-specificity http://www.anaesthetist.com/mnm/stats/roc/
ROC for all patients • test to detect presence of eyelash reflex. • all indices very good • high sensitivity • high specificity
grade1 grade 2 grade 3
Bispectral Index available circa 1996 Improved platform XP recent FDA approval– to reduce awareness 19% increased sales per year for 5 years Profit this year UK use of depth monitoring set to increase
maximum sensitivity = 72.7% maximum specificity = 78.5% cut off point = 99.4%
Summary.. 1. BIS/Entropy – can be used in patients after subarachnoid haemorrhage. 2. Grade 1 and grade 2 patients works well. 3. Grade 3 patients (rarer) possibly some fall off in performance. In our study, BIS performed better than Entropy indices. But Entropy; a. Still functions very well. b. May give advanced warning of light anaesthesia.
acknowledgements; Keith Kelly – consultant anaesthetist WGH. Peter Andrews – consultant anaesthetist WGH. Neuro anaesthetists/radiologists – WGH. Theatre/angio suite staff WGH. Lee Dalgety – Datex-Ohmeda. F Duncan.
x rays position
A Comparison of Frontal and Occipital Bispectral Index Values Obtained During Neurosurgical Procedures Toshie Shiraishi, MD, Hiroyuki Uchino, MD, Takeshi Sagara, MD, and Nagao Ishii, MD Department of Anesthesiology, Tokyo Medical University Hachioji Medical Center, Tokyo, Japan
25 patients – for clipping unruptured cerebral aneurysms propofol/fentanyl anaesthesia correlation r2 = 0.9682 between occipital and frontal but maintained at 40-60, little data on how monitors behaved outwith this area
properties of ideal anaesthetic depth monitor • Indicates the stage during light anaesthesia preceding conscious awareness • Real time presentation of results. • Closely reflects changing concentrations of anaesthetic agents and monotonic. • Able to stage the depth of anaesthesia for all anaesthetics on a common scale. • Practical and cost effective. lots of buts however…
ideal anaesthetic depth monitor, showing interindividual variability, but maintains monotonicity
ROC data for BIS RE SE. To detect difference between “anaesthesia” and awake/eyelash reflex present.