Download
1 / 12
120 likes | 224 Views
MRCPath Part 2 - 2006 Lucy Jenkins NE Thames Regional Molecular Genetics Great Ormond Street Hospital. MRCPath Part 2. GOSH Aug 2000 after 9 yrs in Leeds Deafness services Pressure to sit Pt 2 Topic? Casebook or dissertation?. MRCPath Part 2. Pendred syndrome service

E N D
MRCPath Part 2 - 2006 Lucy Jenkins NE Thames Regional Molecular Genetics Great Ormond Street Hospital
MRCPath Part 2 • GOSH Aug 2000 after 9 yrs in Leeds • Deafness services • Pressure to sit Pt 2 • Topic? • Casebook or dissertation?
MRCPath Part 2 • Pendred syndrome service • Choice of submission: • Publications? • Casebook? • Planned dissertation • – Some small cases (important) • - Techniques from developing services • - Audit of referrals / mutations detected / pick up rates
MRCPath Part 2 • Submission of Proposal: Feb 2003 • Dissertation on setting up services for the most common causes of syndromic (Pendred) and non-syndromic (connexin 26) hearing loss • March 2003 proposal accepted • 12 months until written submission • Continued with deafness services – ‘gathering data’
MRCPath Part 2 • Write up on maternity leave !? • Back to work Apr 2005 • Planned to submit by end of year • College changed format – Spring exam only • My Deadline for submission – August 2005 to allow 6 months for marking
MRCPath Part 2 • Referred to & tried to follow proposal • Introduction to deafness (types of HL, loci, genes etc.) • Connexin 26 background, strategy & cases chosen to demonstrate AD, syndromic HL, heterogeneity & pathogenicity • Pendred syndrome background, testing strategy & cases to demonstrate IBD, heterogeneity, and mutations in cis • Results – no. of patients tested, mutations detected, pick-up rates, polys, images of data • Discussion & further work • Appendices for methods, references and useful info (MIM codes, accession numbers, websites). • Submitted August 2005
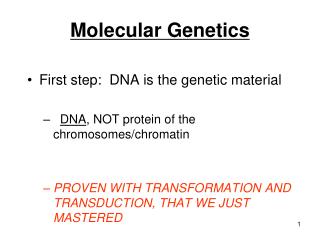
CASE 1: To demonstrate connexin 26 as a cause of non-syndromic dominant hearing loss. AE was referred for connexin 26 mutation analysis with U shaped moderate to severe hearing loss (see audiogram below) that is suggestive of dominant inheritance. DHPLC RESULTS FOR AE AE Normal control 250 500 1000 2000 4000 8000Hz 10 20 30 40 50 60 70 80 90 100 110 dB AE was analysed according to the connexin 26 strategy and found to have c.551G>A (p.Arg184Gln) only. This mutation has previously been reported to be dominant acting (25). Key: Connexin related deafness Red = GJB2 genotype R184Q = p.Arg184Gln N = Normal Normall N R184Q / N AE R184Q / N N R184Q / N Profound Left Right R184Q / N R184Q / N Additional family members were referred (see pedigree) and results were consistent with p.Arg184Gln segregating with the hearing loss. This indicated autosomal dominant inherited hearing loss in AE’s family, however further family members were requested for clarification as the only hearing relatives tested were related by marriage. Additional family members have not yet been referred.
MRCPath Part 2 • Oct 2005 – Grade B • Resubmitted a week later with minor amendments • - detail on commissioning services (gene dossier) • - table of deafness genes (NSHL & SHL) • Grade A - Nov 2005
MRCPath Part 2 • Applied for exam Jan 2006 • Letter accepting application. Date & examiners confirmed later (Graham Taylor & David Robinson) • Exam March 2006
MRCPath Part 2 Career so far Mutations we can and can’t detect (deep intronic, promoter…) New technologies for mutation detection What is important for a mutation scanning technique (TGCE / Lightscanner / CSCE / Seq) Large deletions recently reported as polys (Nat Genet ‘06) – what effect How would you distinguish if part of a tumour progression / a poly Molecular Cytogenetics – array CGH & subtelomeres Views on QFPCR vs. karyotyping
MRCPath Part 2 • Mental retardation, who to test & how? • How do you know your strategy is right? • Just DD on card, would you test? • 3yr old for FX – would you test? • Setting up a new rare disease service, discussion on gene dossiers • What if someone wanted testing who had an aunt with mutation found in a research lab abroad • Reasons for females manifesting X-linked disorder • Sample mix up – delF508 typed N - what would you do? • Agenda for change - impact on skill mix
In summary: • Advice helping to decide type of written submission • Royal College Guidelines • DEADLINE • Advice with dissertation once started from Mentor • For exam: Recent publications and issues