Download
1 / 20
200 likes | 263 Views
Options for Teaser Bull Surgical Procedures. Kathy Whitman, DVM, MS Great Plains Veterinary Educational Center. Gomer bull selection. Purpose: heat detection, synchronization, estrus induction Mature, virgin bulls, free of STDs and other biosecurity risks

E N D
Options for Teaser Bull Surgical Procedures Kathy Whitman, DVM, MS Great Plains Veterinary Educational Center
Gomer bull selection • Purpose: heat detection, synchronization, estrus induction • Mature, virgin bulls, free of STDs and other biosecurity risks • Structurally sound and sufficient size • Libido with limited human risk • Additional history?
Surgical preparation • 24-48 hour fast for ruminating bovines • Physical exam • Does he have nuts?????? • Anesthetic risk • Ancillary testing • PCV/TP • Anesthesia/analgesia/antibiotics • Positioning • Generally dorsal recumbency • Appropriate padding • Tilted for surgeon preference • Well restrained • Protect eyes
Surgical preparation • Aseptic procedure!!! • Scrub and prep like you’re a surgeon and it matters • Clip-flank to flank, scrotum to xyphoid • Aseptic scrub, +/- drape • Clamp or purse string sheath to minimize urine contamination • Instrumentation/surgery pack • Sterile • Plan for worst case scenario-what would you require? • Suture choice • Scarring is good in most cases-do you want it to resorb? • Don’t put it where it’s not needed-ex. epididymectomy • Suture removal?
Surgery similarities • Patient positioning • Patient preparation • Be confident in making incision • Use scissors-better control, better hemostasis • Control hemorrhages as needed-take time to ligate • Limit time, trauma, and contamination • Reduce dead space if necessary • Continuous pattern for skin is sufficient • Sexual rest is required in all situations-up to 6 weeks if uncomplicated
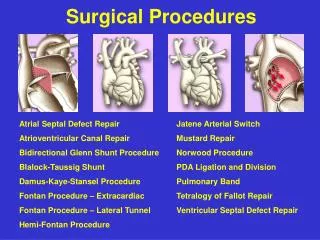
Various surgical methods • Epididymis • Epididymectomy • Iatrogenic necrosis • Vas deferens • Vasectomy • Vasostomy • Penis • Penectomy • Penopexy • Phallectomy • Translocation
Epididymis • Epididymectomy • Can be performed standing with local block • Use in combination with other procedures • Emasculotome • A problem if proper clamp is not applied-per spermatic cord • Maintain libido? • Caustic procedures • Ethical? • Humane?
Vas deferens • Vasectomy • Ligation and transection of the vas (ductus) deferens • Vasostomy • Transection and reattachment to exterior • Allows for evacuation of semen • Tedious and no clear advantage over vasectomy
Vas deferens-Vasectomy • Performed standing, lateral, or dorsal recumbency • Preparation of scrotal neck with local block • 1-2 in vertical incision in neck of scrotum, proximal to testicle • Extend into tunica dartos to expose spermatic cord • Blunt dissection to continue through tunica vaginalis to isolate ductus deferens • Visualize cremaster, vein, and artery-AVOID ligating/transecting these • Two ligatures (absorbable, monofilament) 2 in apart, transect • Close tunics and skin
Penis/prepuce • Penopexy (penile fixation) • Penis is fixed to prevent extension-high and low options • Penectomy • Urethrostomy with penis removal-high and low options • Phallectomy • Amputation of distal penis • Translocation • Tunneling • Z-plasty
Penopexy (low) Surgical prep and line block Identify preputial reflection Use of a vaginal speculum to protect penis and identify reflection is useful Incise caudal to reflection, lateral to penis Using blunt dissection, isolate a 4-6 cm section of penis Place 3 interrupted sutures (non-absorbable, #3) through the tunica albuginea of the dorsal penis Again, avoid important structures Secure to the linea alba Simple interrupted to close skin Rest 2-3 weeks
Penopexy Body Wall Linea alba Tunica albuginea Non-absorbable suture, uninterrupted simple continuous
Penectomy/Phallectomy Standing procedures Use caudal epidural and pudendal blocks +/- Light sedation Keep urethra patent
Translocation-Tunneling Surgical prep and line block, block flank incision site Circumferential incision around prepuce extending caudally to base of the scrotum-speculum as a guide and contamination control or purse string Circular incision and removal of tissue cranial to flank fold (45 from distal aspect of midline incision) Dissect penis within prepuce until it is freed from underlying tissues Using uterine forceps or instrument of length, create a tunnel from the distal end of the midline incision Place sterile sleeve or speculum thru tunnel Draw penis through sterile apparatus and bring through flank hole Suture subcutis (if needed) and skin
Surgical concerns… • Bull waking up… • Hopefully you tied good knots… • Re-dosing is okay, do not compromise good technique for speed • Not sure where to cut or how to proceed? • When a problem presents itself, the time for preparation has passed • Stop, breath, ask questions • Bleeders • Unclamp yourself and clamp the bleeder-ligate as needed • Address this issue up front-surgical field will be poor if you ignore • Puckered skin when suturing • Remove “dog ears” when seal is complete • Remove suture and begin again • We’ll tease you if it’s ugly, we’ll be upset if it comes apart
Post surgical care • Return to recumbency should be rapid, but don’t rush to get them up • <30 min standing • Monitor for excessive bleeding and/or swelling • Appetite should be back to normal relatively quickly if pain management is appropriate and no complications
Post surgical problems • Typically minimal with z-plasty • Abscess, dehiscence, systemic infection, etc. • Iatrogenic urinary obstruction • Intromission still possible… • Discussion all potential issues with owner!!!!