Download
1 / 47
470 likes | 563 Views
Elements of innate and acquired immunity. E. coli bacteria adhering to the surface of epithelial cells of the urinary tract. Figure 2.1 The developmental pathway of various cell types from pluripotential bone marrow stem cells. Neutrophil.

E N D
Elements of innate and acquired immunity
E. coli bacteria adhering to the surface of epithelial cells of the urinary tract
Figure 2.1 The developmental pathway of various cell types from pluripotential bone marrow stem cells.
Neutrophil This granulocyte has very tiny light staining granules (the granules are very difficult to see). The nucleus is frequently multi-lobed with lobes connected by thin strands of nuclear material. These cells are capable of phagocytizing foreign cells, toxins, and viruses. When taking a Differential WBC Count of normal blood, this type of cell would be the most numerous. Normally, neutrophils account for 50-70% of all leukocytes. If the count exceeds this amount, the cause is usually due to an acute infection such as appendicitis, smallpox or rheumatic fever. If the count is considerably less, it may be due to a viral infection such as influenza, hepatitis, or rubella.
Eosinophil This granulocyte has large granules (A) which are acidophilic and appear pink (or red) in a stained preparation. This micrograph was color enhanced to illustrate this feature. The nucleus often has two lobes connected by a band of nuclear material. (Does it looks like a telephone receiver?) The granules contain digestive enzymes that are particularly effective against parasitic worms in their larval form. These cells also phagocytize antigen - antibody complexes. These cells account for less than 5% of the WBC's. Increases beyond this amount may be due to parasitic diseases, bronchial asthma or hay fever. Eosinopenia may occur when the body is severely stressed.
Basophil The basophilic granules in this cell are large, stain deep blue to purple, and are often so numerous they mask the nucleus. These granules contain histamines (cause vasodilation) and heparin (anticoagulant). In a Differential WBC Count we rarely see these as they represent less than 1% of all leukocytes. If the count showed an abnormally high number of these cells, hemolytic anemia or chicken pox may be the cause.
Lymphocyte The lymphocyte is an agranular cell with very clear cytoplasm which stains pale blue. Its nucleus is very large for the size of the cell and stains dark purple. This cell is much smaller than the three granulocytes (which are all about the same size). These cells play an important role in our immune response. The T-lymphocytes act against virus infected cells and tumor cells. The B-lymphocytes produce antibodies. This is the second most numerous leukocyte, accounting for 25-35% of the cells counted in a Differential WBC Count. When the number of these cells exceeds the normal amount, one would suspect infectious mononucleosis or a chronic infection. Patients with AIDS keep a careful watch on their T-cell level, an indicator of the AIDS virus' activity.
Monocyte This cell is the largest of the leukocytes and is agranular. The nucleus is most often "U" or kidney bean shaped; the cytoplasm is abundant and light blue (more blue than this micrograph illustrates). These cells leave the blood stream (diapedesis) to become macrophages. As a monocyte or macrophage, these cells are phagocytic and defend the body against viruses and bacteria. These cells account for 3-9% of all leukocytes. In people with malaria, endocarditis, typhoid fever, and Rocky Mountain spotted fever, monocytes increase in number.
Macrophages are 5 - 10 fold larger than monocytes, and contain more organelles, especially lysosomes. Alveolar macrophages in the lung Histiocytes in connective tissues Kupffer cells in the liver Mesengial cells in the kidney Microglial cells in the brain Osteoclasts in bone
- Langerhans cells - Interstitial dendritic cells - Interdigitating dendritic cells - Circulating dendritic cells (veiled cells) SEM micrograph of follicular dendritic cells showing long, beaded dendrites
Phagocytosis and processing of exogenous antigen by macrophages
Erythrocyte The background cells in this micrograph are erythrocytes (red blood cells). These cells are non-nucleated, biconcave discs that are filled with hemoglobin. The primary function of these cells is to carry oxygen from the lungs to the body cells. Woman usually have 4-5 million erythrocytes per cubic millimeter of blood, men have 5-6 million. If this number is considerably higher, polycythemia may be the cause. If the number is considerably less, the person has anemia.
Sickle cell anemia is an inherited condition which results in some erythrocytes being malformed. The gene for this condition causes the hemoglobin to be incorrectly formed, which in turn causes some erythrocytes to take on a crescent shape. These cells are not able to carry adequate amounts of oxygen to cells.
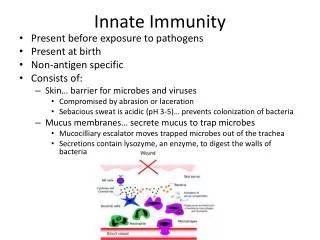
Phagocytic defenses Phagocytes : - class of cells capable of ingestion (engulfment) & destruction of microorganisms - recruited to site of inflammation - two cell types 1) neutrophil (PMN) - 1st to accumulate around invaders & initiate phagocytosis 2) tissue & blood borne macrophages (mononuclear phagocytes - migrate to site & initiate phagocytosis
Figure 2.2 Endocytosis and phagocytosis by macrophages.
Figure 2.3 A polymorphonuclear leukocyte (surrounded by erythrocytes in a blood smear) with a trilobed nucleus and cytoplasmic granules. (Photograph courtesy of Dr. A. C. Enders, School of Medicine, University of California, Davis).
Figure 2.4 A scanning electron micrograph of a macrophage with ruffled membranes and a surface covered with microvilli. (Photograph courtesy of Dr. K. L. Erickson, School of Medicine, University of California, Davis)
Figure 2.5 Schematic representation of NK cell inhibitory receptors and killing.
Inflammation - Def: Tissue reaction to infection or injury, characterized by erythema, swelling, heat, pain & loss of normal tissue function - Necessary for proper functioning of host defenses Erythema : due to increased blood flow Swelling : due to increased extravascular fluid & phagocytic infiltration Heat : due to increased blood flow & pyrogens Pain : due to tissue distruction & irritation of sensory nerve receptors
Figure 2.6 The distribution of lymphoid tissues in the body.
Roles of various lymphoid tissues in immune system function Generatingbone marrowsource of lymphocytes stem cells Regulatingthymus, BMsites of regulation of productionbursa lymphocyte development Providingspleen, BMsite of lymphocyte-Ag environmentlymph nodesinteractions for cell-Ag tonsils interactionPeyer’s patch
Primary lymphoid organs- maturation of lymphocytes- removal of self-reactive lymphocytes • Thymus • differentiation of T cell lymphocytes • Bone Marrow (bursa of Fabricus in birds) • differentiation of B lymphocytes
Thymus • 1. Lymphoepithelial organ • 2. Differentiation of T lymphocytes • 3. Only 5 - 10% of maturing T cells survive • 4. Size • 1) relative size greatest in newborn • 2) absolute size greatest in puberty • 3) atrophy after puberty • 5. Maturation of T cells - mainly during fetal • development and for a short time after birth
Figure 2.7 The cellular organization of the thymus.
Thymus & tolerance - Tolerance results if host lacks T cells with receptors specific for Ag - Range of T cell receptors (TCR) determined in thymus BM stem cells React w/ self MHC Positive selection Thymocyte proliferation React w/ “self” thymocytes Negative selection Apoptosis
Secondary lymphoid organs- angen-induced activation of lymphocytes • Spleen (filters blood) • Lymph nodes (filter lymph) • Mucosa-associated lymphoid tissue (MALT) • Gut-associated lymphoid tissue (GALT) • Peyer’s patches, tonsils, appendix, ……. • Bronchus -associated lymphoid tissue (BALT) • diffused aggregates of lymphocytes
Spleen - Removes Ag & aged blood cells - Stores RBC & platelets - Site for Ab production & effector T cells - Consists of red pulp - storage of RBC & Ag trapping white pulp - immune response
Rich in lymphocytes Erythrocytes & macrophages Figure 2.8 Schematic views and light micrograph of a section of spleen.
B cells Macrophages T cells Derived from follicles after Ag stimulation
Response of spleen to antigen Ag trapped in spleed macrophages in marginal zone, red pulp primary follicles in white pulp Ab producing cells in primary follicles germinal center in primary follicles
Figure 2.9 (A) A diagrammatic representation of a section of a lymph node. (B) A section through a lymph node showing the capsule, the subcapsular sinus, the medulla (upper left), and the cortex with secondary follicles containing germinal centers. Also shown (upper right) is a follicle without a germinal center.
Structure of M cells and production of IgA at inductive sites
Figure 2.10 Circulation of lymph and fate of antigen following penetration through (1) the bloodstream, (2) the skin, and (3) the gastrointestinal or respiratory track.
Figure 2.11 The interrelationship between innate and acquired immunity.