Download
1 / 53
570 likes | 857 Views
Kidney Introduction Pathogenesis of glomerular diseases. Objectives. By the end of this session the student should be able to: List the major clinical presentation of disorders of the kidney. Describe the anatomical components of the kidney and list the major diseases of each.

E N D
Objectives • By the end of this session the student should be able to: • List the major clinical presentation of disorders of the kidney. • Describe the anatomical components of the kidney and list the major diseases of each. • List and describe the types of immune mechanisms in glomerular diseases.
Introduction • Kidney function • Components of Blood • RBC • WBC • Plasma (water, electrolytes, protein) • Anatomical/Histological components: • Glomeruli • Tubules • Interstitium • vessels
Glomeruli Glomerulonephritis Primary Secondary Chronic Tubulointerstitium Acute tubular necrosis Pyelonephritis Acute chronic Vessels Nephrosclerosis Benign Malignant Urinary obstruction Stones Hydronephrosis Cystic diseases of the kidney Tumors Diseases of the kidney
Renal dysfunction • Urea, creatinine • Azotemia (high urea, creatinine) • Pre renal • Renal • Post renal • Uremia (azotemia+ clinical features) • Features of uremia
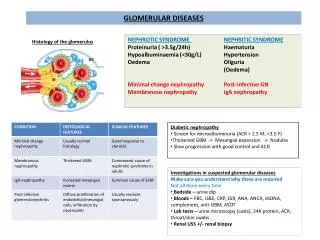
Major clinical presentations • Acute nephritic syndrome • Gross hematuria, mild-moderate proteinuria, hypertension, azotemia, edema • Nephrotic syndrome • Heavy proteinuria (>3.5g/day), hypoalbuminemia, edema, hyperlipidemia, lipiduria • Asyptomatic hematuria or proteinuria
Major clinical presentations • Rapidly progressive glomerulonephritis • Acute renal failure • Chronic renal failure • UTI urinary tract infection • Renal colic (stones) • Obstruction • Mass lesion
Kidney Biopsy • Send fresh • Routine processing • Immunoflourescence (IF) • Electron microscopy (EM) • Light microscopy (formaline fixed)
A 47-year-old black male truck driver presents to the emergency room with intractable nausea and vomiting, dyspnea on exertion, and dizziness. The nausea began about two weeks prior to admission; vomiting has occurred within the last few days. The chest pain has been present for only 2-3 days and is described as retrosternal, burning, and worse on inspiration. There is no history of medication or toxin exposure. His past medical history is positive for hypertension diagnosed 14 years ago with no follow-up. He has smoked 1 ppd for 27 years.
On physical examination, he is a thin, black man in moderate distress. His blood pressure is 160/120, temperature 36.7°C, pulse 100 (nl 60-100/min). His skin is pale with numerous areas of bruising. Lung exam reveals bilateral rales to the mid lung fields, and cardiac exam reveals muffled heart sounds, a friction rub, and a I/VI systolic ejection murmur. Chest x-ray shows moderate cardiomegaly with increased pulmonary vascular markings and hazy obliteration of the lower lung bases. Abdominal ultrasound examination shows a right kidney size of 7 cm (nl approx. 10 cm) and a left kidney size of 6.8 cm without evidence of pelvicalyceal dilation.
Urinalysis: • protein - 1+ • blood - 1+ • glucose - neg • casts - neg • bacteria - neg
WBC: 6,700/mm3 • Platelets: 250,000/mm3 • Hematocrit: 26% • Creatinine: 200 mmol/L (high, normal <120) • BUN: 215 mg/dL (high, normal <25) • Calcium: 6.2 mg/dL (low, normal 8-10mg/dl) • Uric Acid: 16.5 mg/dL (high, normal 5-7) • Cardiac markers of MI: negative
An echocardiogram reveals a moderate amount of fluid around the heart. A pericardiocentesis is performed, and 250 cc of serosanguineous fluid is removed. An urgent request for hemodialysis is made, and the patient is dialyzed with some relief in his breathing and chest pain. However, the next morning, the patient complains of abdominal pain and passes several melanotic stools, followed by gross blood. Hypotension and arrhythmias follow, and death supervenes. An autopsy is performed.
What are the possible causes of this appearance of the kidneys?
Describe the four compartments (glomeruli, tubules, interstitium, and vasculature)
Discussion • Hypertension • Chronic Renal Failure • Uremia • Urinalysis • Blood work • Kidney findings • Secondary hyper parathyroidism
Glomerulus • Structure • Filtering membrane • 1. Endothelial cells • 2. GBM glomerular basement membrane • 3. Visceral epithelium • GFR: glomerular filtration rate • Mesangium • Permeablility • Water, albumin • Size, charge
Glomerular disease • Primary • Seconday • Hereditary
Glomerular disease • Primary • Minimal change GN • Membranous GN • Focal segmental GS • Membranoproliferative GN • Diffuse proliferative GN • Crescentic GN • Seconday • SLE, DM, Amyloidosis, Goodpasture, vasculitis • Hereditary • Albort syndrome
Pathogenesis of Glomerular Disease Immune disorder Kidney involvement Injury by inflammation and other mediators Glomerular dysfunction
Pathogenesis of Glomerular Disease Immune disorder • Circulating immune complex • Immune complex formation • Cell-mediated Glomerular dysfunction
Pathogenesis • 1. Circulating Immune complex nephritis (type III hypersensitivity) • Antigen is not glomerular origin • Intrinsic- SLE • Extrinsic- Poststreptococcal GN, HepB, Malaria • Ag-Ab complex is trapped in glomeruli • Complement activation • injury
Pathogenesis • 1. Circulating Immune complex nephritis (type III hypersensitivity) • Morphology: • IF: deposits (glomerular) • EM: electron-dense deposits (mesangial, subendothelial, subepithelial) • Proliferative: leukocytes, endothelial, mesangial, epithelial
Pathogenesis • 1. Circulating Immune complex nephritis (type III hypersensitivity) • What happen • Short lived Ag-Ab complex---- Recovery • Repeated Ag-Ab complex------- chronic GN
Pathogenesis of Glomerular Disease Immune disorder • Circulating immune complex • In-situ Immune complex formation • Cell-mediated Glomerular dysfunction
Pathogenesis • 2. In-situ Immune complex nephritis • In-situ • Intrinsic • Extrinsic/planted
Pathogenesis • 2. In-situ Immune complex nephritis • Anti-GBM • Goodpasture syndorme • In human: auto antibodies • Pathology: • Severe glomerular damage • Cresentic GN • Ag: alpha3 chain of collagen type IV • (Rabbits Masugi Nephritis) injury to rats by antibodies of rabbit • IF: linear deposits
Pathogenesis • 2. In-situ Immune complex nephritis • Haymann Nephritis: • Immunizing rats to proximal tubular brush border • IF: granular deposits of Ig and complement along the GBM • Ag (megalin) on visceral epithelial cells • Result in membranous GN
Pathogenesis • 2. In-situ Immune complex nephritis • Planted antigen • DNA • Bacterial products (groupA strep) • IgG/complex • IF: granular pattern
Pathogenesis of Glomerular Disease Immune disorder • Circulating immune complex • In-situ Immune complex formation • Cell-mediated Glomerular dysfunction
Pathogenesis • Cell mediated Immune GN • Sensitized T cells • suspected
Pathogenesis of Glomerular Disease Immune disorder • Circulating immune complex • In situ Immune complex formation • Cell-mediated Glomerular dysfunction
Pathogenesis of Glomerular Disease Immune disorder Kidney involvement Injury by inflammation and other mediators Glomerular dysfunction
Mediators of Immune Injury • Mediators • Cells • Plasma products
Mediators of Immune Injury • Mediators • Cells • Neutrophils • Proteases, oxygen free radicals • Monocytes • Platelets • Epithelial cells • Plasma products
Mediators of Immune Injury • Mediators • Cells • Plasma products • Direct cytotoxicity by Ab • Fibrin related products • Complement activiation • C5-C9 membrane attack complex
Epithelial cell injury • Ab to visceral epithelium • Toxins • Cytokins • Loss of foot processes, vacuolization, detachment • proteinuria
Pathogenesis of Glomerular Disease Immune disorder Kidney involvement Injury by inflammation and other mediators Glomerular dysfunction