Download

1 / 21
210 likes | 438 Views
Familial Mediterranean fever (FMF). Dr. Müge Bıçakçıgil Kalaycı. Familial Mediterranean fever. R ecurrent, short-lived episodes of fever accompanied by peritoneal, pleural, or arthritic inflammation . the mechanisms leading to the clinical manifestations of the disease are still unknown.

E N D
Familial Mediterranean fever(FMF) Dr. Müge Bıçakçıgil Kalaycı
Familial Mediterranean fever • Recurrent, short-lived episodes of fever accompanied by peritoneal, pleural, or arthritic inflammation. • the mechanisms leading to the clinical manifestations of the disease are still unknown
The inheritance of familial Mediterranean fever • The disease may become manifest as early as during the first year of life, although in most cases onset is later. • In two-thirds of patients the first manifestations appeared during the first decade of life; by the end of the second decade 90 per cent are affected. • Only rarely is the onset delayed beyond the age of 40.
PATTERN OF INHERITANCE • Autosomal recessive trait • FMF is most prevalent in individuals of: • Sephardic Jewish (1 in 6 – 8 ) • Armenian (1 in 7 ) • Ashkenazi (1 in 12 ) • Turkish • Arab descent
The FMF gene ( MEFV ) • MEFV is located on the short arm of chromosome 16 • MEFV encodes a 781 amino acid protein • Sites, 694 and 726, are widely distributed. • M694V is more severe than that of V726A • at least 23 mutations have been identified .
Attacks • The febrile, painful attacks that are the hallmark of the disease are characterized by; • marked elevation of body temperature, • acute inflammation of the peritoneum, synovia, or pleura, • a duration of 12 to 48 h, and • complete health between attacks . • Repeated attacks at irregular intervals and in an unpredictable sequence
Abdominal attack • The most frequent manifestation • experienced by 90 per cent of patients • They are marked by the sudden onset of fever (often with chills) • Pain spreading over the entire abdomen from variable points of origin. • Guarding, rebound tenderness, board-like rigidity, distension, and absence of peristalsis appear. • Multiple, small fluid levels in the small bowel on radiography • Suggest an acute abdominal catastrophe.
Abdominal attack • After 6 to 12 h the signs and symptoms recede, and within 24 to 48 h the attack is usually over, leaving the patient as well as before. • Organization of the exudate may result in fibrous adhesions, • mechanical ileus • sterility in some affected women .
pleural attack • 45 % of patients, and in 5 % it was the presenting sign . • abrupt onset, rapid resolution, and unpredictable recurrence. • Breathing is painful and breath sounds are diminished on the affected side. • small exudate in the costophrenic angle, which is difficult to aspirate and which resolves within 48 h.
Pericarditis- • a rare feature of familial Mediterranean fever. • No permanent sequelae have been reported. • Muscle pains (20%) • lasts from a few hours to 1 to 2 days, and • subsides with rest or non-steroidal anti-inflammatory drugs.
articular attack • the second most common form of attack. (75%) • Arthritic attacks may recur for years as the only feature of the disease, before other forms appear . • Large joints are involved, particularly those of the lower extremities. • In two forms: • acute, or • chronic and protracted.
In the acute form: • the onset is abrupt, • fever ranges from 38 to 40°C, and • the affected single joint is tender, swollen, and held immobile • The signs and symptoms usually peak in 1 to 2 days and then gradually subside, leaving no residue. • The attacks can sometimes be precipitated by minor trauma or effort, such as prolonged walking. Synovial effusion is often demonstrable. • Resolution of a short attack can occur in as soon as 2 to 3 days, but more commonly takes a week and sometimes nearly a month.
Chronic-protracted attacks (5%) • persist for more than a month. • Usually the hip or knee are involved , • the joint remains markedly swollen and painful, presenting a picture of chronic monoarthritis or chronic oligoarthritis. • After several weeks or months, sometimes even after a year or more, the pain subsides spontaneously. • During such protracted attacks in a joint, short attacks involving other joints, the abdomen, or chest may occur .
Erysipelas-like erythema (11%) • one of the most characteristic manifestations of FMF. • usually combined with arthritis. • Rather sharply bordered red patches, hot, tender, and swollen, and 10 to 35 cm2 in area, appear on the skin of the lower extremities. • They are usually located between the knee and ankle, or on the dorsum of the foot or ankle region, and are also accompanied by abrupt elevation of body temperature and last about 24 to 48 h .
Orchitis • an acute, unilateral, painful swelling and redness of the testis • it subsides spontaneously after 12 to 24 h, without anatomical residue .
Mild splenomegaly of 1 to 4 cm, unrelated to amyloidosis. • Haematuria, sometimes only microscopic. • Amyloidosis is major cause of mortality in FMF.
Tel-HashomerDiagnostic criteria Majorcriteria 1.Painful inflammatory manifestations in the abdomen, chest, joints, or skin, associated with the fever. 2.Nephropathicamyloidosis. 3.Dramatic response to continuous colchicine treatment in abolishing or reducing febrile attacks Minorcriteria 4.Short attacks of fever recurring at irregular intervals. 5.Familyhistory 6. Erysipelaslikerash Diagnosis- 2 majoror 1 major 2 minorcriteria
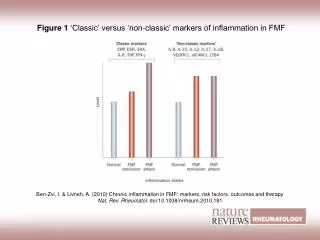
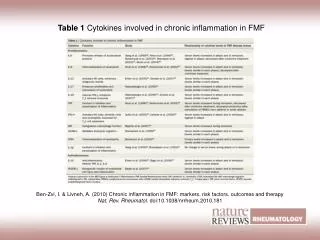
Laboratory findings • non-specific. • The erythrocyte sedimentation rate is accelerated and • acute-phase proteins such as a2-globulin and fibrinogen are increased, especially during attacks, but also in between • Leucocytes increased • Crp and ESR elevated
Laboratory findings • Serum amyloid A is raised • acute-phase protein • the familial Mediterranean fever (FMF) gene located on the short arm of chromosome 16
Treatment-to prevent attacks • Daily prophylactic treatment with colchicine • Treatment is started with 1 mg colchicine/day, regardless of age or severity of attacks. • This dose is increased if necessary to 1.5 to 2 mg, until remission from attacks is achieved. • Continuous prophylactic treatment with colchicine in patients inhibits the development of nephropathic amyloidosis .