Download
1 / 30
300 likes | 339 Views
HISTAMINE & ANTAGONISTS. Histamine is a major mediator of Inflammation Anaphylaxis Gastric acid secretion Also plays a role in neurotransmission. Histamine 5-HT Angiotensin, BK, Kallidin PG, Leukotrienes Cytokines Histamine has no clinical application in the treatment of disease

E N D
Histamine is a majormediator of • Inflammation • Anaphylaxis • Gastricacidsecretion Alsoplays a role in neurotransmission
Histamine • 5-HT • Angiotensin, BK, Kallidin • PG, Leukotrienes • Cytokines • Histamine has no clinical application in the treatment of disease • The receptor agonists and antagonists Autacoids
Tissues contain Substances (when released by various stimuli) Reddening of skin Pain or itching Bronchospasm Many of these substances are also present in nervous tissue and have multiple functions Histamine and serotonin are biologically active amines, function as neurotransmitters, present in nonneural tissues and have complex physiologic and pathologic effects, have multiple receptors, released locally→autocoids It is synthesized in 1907 and later isolated from mammalian tissues.
CHEM & PK • H occurs in plants and animal tissue, a component of some venoms and stinging secretions • H is formed by decarboxylation of the aa L-histidine by histidine decarboxylase • Once formed H is either stored or rapidly inactivated
CHEM & PK Although H is found in most tissues, it is very unevenly distributed Most tissue H is sequestered and bound in granules in mast cells or basophils. Bound form is inactive, but many stimuli can trigger the release of mast cell H Mast cells are especially rich at sites of potential tissue injury-nose, mouth, and feet, internal body surfaces and blood vessels
CHEM & PK Non-mast cell H is found in several tissues, including the brain, where it functions as a neurotransmitter. It is also found in enterochromaffin-like cell of the fundus of the stomach.
STORAGE AND RELEASE OF HISTAMINE Inhumanmastcellsandbasophils, storagegranulescontain H complexedwithheparin (sulfatedpolysaccharide) orchondroitinsulfate (acidic protein). • Immunologicrelease: IfmastcellsandbasophilsaresensitizedbyIgEantibodiesattachedtotheirsurfacemembranes, theydegranulatewhenexposedtotheappropriateantigen ATP, andothermediatorsarereleased as well
PATHOPHYSIOLOGY OF THE IgE-MEDIATED HYPERSENSITIVITY REACTION Requires energy and calcium
CHEMICAL AND MECHANICAL RELEASE B. Chemical & mechanical release Certain amines, including drugs such as morphine and tubacurarine, can displace H from the heparin-protein complex within the cells. This type of release does not require energy and is not associated with mast cell injury or degranulation.
CHEMICAL & MECHANICAL RELEASE Loss of granules from the mast cell will also release H Chemical 48/80 specifically releases H from tissue mast cells by an exocytotic degranulation process requiring energy and calcium Very little H is excreted unchanged → conversion to N-methylhistamine, methylimidazoleacetic acid and imidazoleacetic acid
PHARMACODYNAMICS H exerts its biological actions by combining with specific cellular receptors located on the surface membrane H1, H2, H3 & H4, no subtypes All 4 type receptors types have been cloned, they are coupled with G proteins
TISSUE AND ORGAN SYSTEM EFFECTS OF H Nervous System Powerful stimulant of sensory nerve endings → pain and itching. H1 mediated effect is an important component of urticarial response and reactions to insect and nettle stings. H1 and H3 →appetite and satiety antipsychotics block these receptors Presynaptic H3 modulate release of NT→decrease release Ach, amine, peptide transmitters in brain and peripheral tissues
CV Injection or infusion of H → BP changes →Direct vasodilator action on arterioles and precapillary sphincters Heart→ stimulatory action of H and reflex tachycardia
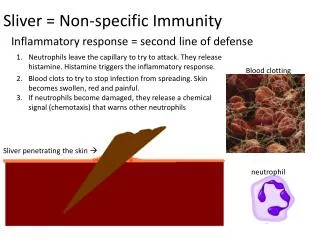
TRIPLE RESPONSE Intradermal injection of H causes a characteristic red spot, edema and flare response that was first described 60 years ago At the site of injection a reddening appears →dilation of small vessels, and precapillary sphincters followed by edematous wheal and a red irregular flare surrounding the wheal (H1). Rubor (redness), calor (heat), dolor (pain), tumor (edema) and loss of function. Flare is caused by an axon reflex H induced edema → the action of amine on H1 receptors in the vessels of the microcirculation, especially the postcapillary vessels
BRONCHIOLAR SMOOTH MUSCLE Causes bronchoconstriction via H1 receptors. Provacative tests using increasing doses of inhaled H are of diagnostic value for bronchial hyperreactivity in patients with asthma or cyctic fibrosis
GI TRACT Causes contraction of intestinal smooth muscle. Powerful stimulant of gastric acid secretion and to a lesser extent of gastric pepsin and intrinsic factor production. H2 receptors on parietal cells and increased adenyl cyclase activity, cAMP and Ca++ concentration.
METABOLIC EFFECTS H might be important metabolic functions H3-receptor knockout mice ↑ food intake ↓ energy expenditure and obesity ↑ blood levels of leptin and insulin Humans???
H1 RECEPTOR ANTAGONISTS Available without prescription. 2nd generation
PK Rapidly absorbed orally, widely distributed, 1st generations readily enter CNS, block autonomic receptors. Onset of action 15-60 min, duration 4-6 h Several 2nd generation agents are metabolized by the CYP3A4 system! Meclizine and several 2nd gen duration12-24h less sedating Pgp
PD • Reversible competitive binding of the H1 receptor some have been shown to be inverse agonists
CLINICAL USES 1.H1 antagonists are often the first drugs used to prevent or treat the symptoms of allergic reactions. Allergic rhinitis and chronic urticaria H1 antag are DOC. In bronchial asthma they are not very effective because other mediators are involved. 2. Numerous allergic dermatoses can be treated 3. In systemic anaphylaxis H1 antihistamines have no primary therapeutic role, cannot control marked hypotension and bronchospasm 4. Little effect on bronchial asthma Sleep aid
5. Chlorpheniramine combined with nasal decongestants and analgesics are used for symptomatic relief of common cold 6.Via CNS action can be used for nausea vomiting, motion sickness
Promethazine, hydroxyzine and diphenhydramine may be used for sedating agents Antihistamines (e.g. diphenhydramine and promethazine) can be used to induce sleep. They are included in various over-the-counter preparations • ADVERSE EFFECTS • Drowsiness, diminished alertness, lethargy and diminished motor coordination • GI disturbances nausea vomiting, epigastric distress uncommon • Tremors, nervousness, irritability, palpitation, tachycardia urinary retention dose related
Overdose of Astemizole terfenadine prolonged QT; interval drug interactions can cause this (No longer available in US) • Loratadine is free from these effects • Blood dyscrazias • Increase CNS effects of barbiturates,opioids, general anesthetics
OTHER ACTIONS BY H RECEPTOR BLOCKERS Sedation Antinausea and antiemetic actions Antiparkinson effect Anticholinoceptor action Serotonin blocker action Local anesthesia
TOXICITY Sedation, antimuscarinic action most common. Less common toxic effects are excitation and convulsions in children, postural hypotension, and allergic responses (which is more common after topical use of H1 antagonists).