Download
1 / 144
1.46k likes | 1.73k Views
Office Management of Personality Disorders (Borderline). Stephen H. McNevin BSc MD FRCPC Personality Disorders Service Providence Care – Mental Health Services Director Division of Psychiatry Health Counseling and Disability Services Queens University

E N D
Office Management of Personality Disorders (Borderline) Stephen H. McNevin BSc MD FRCPC Personality Disorders Service Providence Care – Mental Health Services Director Division of Psychiatry Health Counseling and Disability Services Queens University PGY2 Academic Day Department of Family Medicine Queens University at Kingston August 14 2014
Disclosures • Research or Speakers Funding from • Pfizer • Eli Lilly
Learning Objectives • Become familiar with the presentation of persons with personality disorders in the community setting • Be able to develop an approach to the assessment of personality disorders • Become familiar with effective pharmacological and psychotherapeutic treatments and resources for persons with personality disorder • Learn how to apply good psychiatric management and dialectical behavior therapy principles in day to day care of persons with personality disorders
Take Home Message • Not everyone is bipolar • Radical Acceptance • Know your limits and stick to them • Avoid hospitalization - LISTEN • Medication – is not the solution • Very treatable
The Difficult Patient • The hated patient • The difficult patient • The problem patient • The hard to serve • The difficult to serve • The poorly served
The Difficult Patient ……any patient who causes staff distress or disrupts the health care environment as a result of emotional dysregulation, intolerance of distress, or interpersonal difficulties …. does not need a formal diagnosis of Borderline Personality Disorder but in the context of the stresses of living may regress into similar maladaptive behaviors
Borderline Personality Disorder • A quick overview….
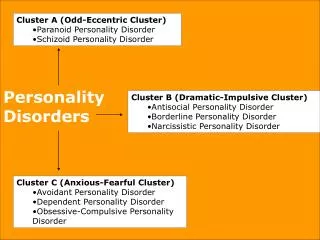
Diagnosis of Personality Disorder • DSM 5 • Definition of a Personality Disorder • Enduring pervasive pattern of inner experience and behavior • Deviates markedly from the expectations of the individuals culture • Manifested in two or more of : • Cognition • Affectivity • Interpersonal functioning • Impulse control
Diagnosis of a Personality Disorder • Clinically significant distress or impairment • Stable long duration (may be masked) • Onset in adolescence or early adulthood • Not better accounted for by another psychiatric condition or drugs or physical illness/injury
Diagnosis of Personality Disorder • DSM V (Section III) a radical restructuring with new definition fewer personality disorders ( 6 vs. 10) a blend of trait domains and facets so every patient gets a diagnosis. No more PDNOS, instead PD-TS. • Borderline PD is left much as it currently is understood even there
Borderline Personality Disorder • 1.6 – 5.9% of general population • Most common P.D. seen clinically • 6% in primary care settings • 10% of psychiatric inpatients • 20% of outpatient psychiatric clinic patients • Women diagnosed 3 times as often as men
Borderline Personality Disorder • Most actively seek treatment for their pain • Excessive anger and fearful wariness of others are symptoms • 10% remit in 6 months, 25% by 12 and 50% by 24 months and rarely relapse • Only a small subgroup require intensive specialized care
Etiology • Many theories and growing evidence to support a synthesis of genetic predisposition and epigenetic factors arising from early stresses and disordered attachment leading to disturbances in serotonin and dopamine systems that in turn lead to affect dysregulation and impulsive aggression…What we see as symptoms are really attempts to adapt a disordered system to the exigencies of everyday life..
Pathology • A core defect in emotion regulation • Reduced serotonergic responsivity …….normal modes of regulating the amygdala are not used… amygdala activity when coupled to prefrontal areas may be less differentiated and not confined to areas usually involved in the expression of emotion..
American Psychiatric Association Clinical Practice Guidelines for Borderline Personality Disorder-2001 While there have been huge advances in the field there has yet to be an official update of these guidelines
Initial assessment Determine the treatment setting Safety evaluation Partial hospitalization Brief inpatient Extended inpatient Comprehensive Evaluation Co morbidities Functional impairments Needs/goals Intrapsychic conflicts Defenses Coping style Stresses APA says to assess patients you need to:
The factors that affect the patient/client Biological Interpersonal Familial Social cultural Consider additional sources of information Medical records Informants who know the patient well APA says
Physical examination Stigmata Co-morbidities Physical causes Psychological assessment Tests (for example) SCL-90 NEO MMPI MCMI Rorschach DAPP TCI Neuro-psych APA says
Laboratory studies Chemistry Hematology B-12, Folate Liver Toxicology Hormonal PTH TSH Sex cetera Diagnostic Imaging X-ray CT PET MRI fMRI EEG QEEG APA says
Axis 1 Co morbidities Mood Bipolar Depression Dysthymia Anxiety GAD PTSD DID Panic Substance Abuse ADHD Developmental Dis Learning Disability Adjustment disorders Sleep Disorders Eating Disorders Bulimia Chronic Pain V Codes etc. APA says
Self Reports Diagnostic CATI,MCMI,MMPI, PDQ,SNAP,WISPI,PAI Trait DAPP-BQ,SNAP, IIP-PD ,NEO-PI,IASR,PACL,TPQ, TCI,SASB-IQ Interviews Diagnostic DIPD,PDE,PDI, SCID-II,SIDP-IV Trait DIB,DIB-R,DIN, PCL-R,PAS,SIFFM Psychological Assessments for Personality
First Impressions • Heart Sink
Assessment in the Trenches • In the assessment and management of patients with Personality Disorders it is essential that you carefully attend to your emotional/gut responses to the person before you You ignore this is at your own peril
Assessment in Family Practice • First Impressions can mislead • Its not just your emotional reaction • You need data and lots of it
Using your feelings • Borderline Personality disordered clients are not the only clients who invoke strong feelings • Listen to your feelings • Use your head in applying those feelings to action/diagnosis
Using your feelings • Splitting • Idealizing/devaluing • Knight in shining armor • Projective identification • Murderous fantasies • Entitlement • Fear • Discomfort
Using your feelings • Your feelings can tell you something is up • Your feelings cannot tell you where you have landed
Using your head • The PDS Introductory ConsultationForm • 1000 and counting
Diagnosis of Borderline Personality Disorder in the World of Family Practice • I RAISED A PAIN mnemonic
I RAISED A PAIN • Identity disturbance • Relationships are unstable • Abandonment is frantically avoided • Impulsivity • Suicidal gestures (attempts ,threats , self harm) • Emptiness, chronic feelings of • Dissociative symptoms • Affective instability • Paranoid ideation under stress • Anger poorly controlled • Idealization alternating with devaluation • Negativistic undermine their own and others efforts
Differential Diagnosis • Borderline Personality Disorder (BPD) …………………..The mental disorder that failed to specialize………..
DiagnosisDifferential Diagnoses • Difficult to tease out PD from Mood Disorders(MD) • Share symptomatology • MD can co-exist with BPD
DiagnosisDifferential Diagnosis • Zimmerman in 2010 reported after a careful gold standard review of patients in a series of studies that: ………almost 25% of previously diagnosed Bipolar Mood Disorder patients really had Borderline PD ……….nearly 40% of patients with BPD had previously been labelled as Bipolar
DiagnosisDifferential Diagnosis ….too many individuals are very invested in their diagnosis, particularly in bipolar disorder, and to try to suggest that they may not have a bipolar disorder is to fight a losing battle.. ..some patients (and doctors) are looking for a magic pill rather than develop the mind set that they need to do some work in therapy…
Diagnosis Rates of Comorbidity Little consensus on rates as result of sample selection, assessment techniques, current versus lifetime disorders • PD plus MD, lifetime estimates 35% - 93% Some concluded that comorbidity is actually very low; a careful history will reveal just PD more often than not (Paris, 2003)
DiagnosisImpact of Comorbid PD on Mood Disorders • Co-occurrence associated with more complex, severe initial presentation • Can result in more modest treatment outcomes for MD • very long term studies demonstrate the treatment of co-morbid depression in BPD is best effected by treating the underlying personality pathology (Gunderson 2014) • Entrenched maladaptive beliefs, emotional lability, rigid defenses, coping strategies, all affect the treatment of other conditions
Differential Diagnosis Mood and PDOverlapping Symptomology Pick a symptom, any symptom . . .
Depressive episode & BPD depressed mood eating, sleep disturbances psychomotor agitation/ retardation, fatigue worthlessness, guilt confusion, difficulty with concentration/thinking recurrent thoughts of death or suicide Manic/hypo episode & BPD elevated mood or irritability grandiosity decreased sleep pressure to keep talking psychomotor agitation flight of ideas or racing thoughts buying, sexual, gambling sprees DiagnosisOverlapping Symptomology
DiagnosisPersonality Disorder PD can often better account for the multiplicity and chronicity of symptoms than can MD diagnosis • Enduring pattern of inner experience and behavior; deviates markedly from cultural expectations; pervasive and inflexible; onset in adolescence or early adulthood; stable over time; leads to distress and impairment • Disturbances in 2+ areas: cognition, affect, interpersonal functioning, impulse control
Differential DiagnosisMajor depressive episodes • Attend to pervasiveness and duration • low mood short-lived, intermittent, sub-clinical, associated with mood instability rather than the extended, continuous low mood of MDE • PD tend to have fewer vegetative symptoms • PD environmentally reactive
Differential DiagnosisManic/hypomanic episodes PD evidence rapid shifts in mood • Moods tend to shift from depression to anger, typically lasting hours to days (Henry et al., 01) • Precipitated by environmental events, usually interpersonal BP continuously elevated mood • Mood tend to shift from depression to elation/ mania, lasting weeks or more, usually no precipitating event
Co-morbid Bipolar and Borderline • Recent advances show these are separate conditions that can co-occur often • They need to both be treated robustly(Gunderson 2014)
Differential DiagnosisPsychotic features • 40% of patients with BPD had quasi-psychotic symptoms (Zanarini, 90) • confusion, difficulty thinking & processing • perceptual aberrations, auditory hallucinations • paranoid symptoms (mildly delusional thoughts) • Symptoms more transient, less pervasive, stress related, with no loss of reality testing with PD
ManagementChallenges in Family Practice • Intense and rapidly changing affect • Verbal and physical aggression • Threats of suicide, self-harm • Testing of rules/limits, missed/late appointments • Helplessness, hopelessness • Substance abuse, dissociation, chronic/acute suicidality, risk-taking • Crisis-driven help-seeking • Blaming of others for feelings, situation
ManagementChallenges [T]he worst and most damaging behaviors of borderline patients are products of the unfortunate relationship between people with borderline personality organization and health care professionals. (Dawson, 93) • Physically and verbally aggressive, self-injure, threaten suicide, tell lies, and collapse on floor with therapists, physicians, other professionals • Regress in hospital
ManagementChallenges “I feel really, really bad. You have to take special care of me and make me safe. No-one ever did that for me when I was a child and you have to!” . . . . . . . . . . Most life situations provide normal feedback to that demand, explicit or implicit. Friends No! Significant Other NO! Employer Health Care System No! NO! Well Okay; We’ll try! Children Rivera, 04
ManagementChallenges [W]e should always consider the possibility that doing nothing might be better than doing something, doing less might be better than doing more . . . (Dawson, 1993) • Can and do make things worse • In part, by assuming responsibility for client’s well-being, directly or indirectly • Systemic problem, bias
ManagementChallenges - Dangerous Currency [U]nfortunately, we provide a context that embraces dangerous currency . . . the accepted currency for interpersonal negotiations with health care institutions includes suicide threats and suicidal behavior, self-harm, mutilation, symptoms of illness, loss of control, conflict over medications, and helplessness.(Dawson, 1993) • In return for concern, attention, connection • A sense of safety and longing to be rescued
Management Challenges • Reaching out / Reaching in Only to the extent that one has access to and acceptance of one’s own personal dynamics can one have a compassionate respectful appreciation of those of others. Nancy McWilliams 1994