Download
1 / 25
260 likes | 518 Views
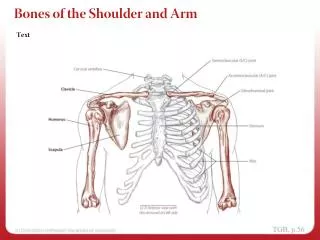
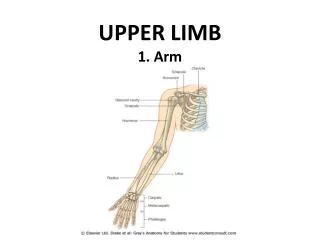
Shoulder and upper arm. CLASSIFICATION The injuries to be described may be classified as follows:. Fracture of the shoulder girdle [1,2] Fractures of the clavicle 3)Fractures of the body of the scapula 4)Fractures of the neck of the scapula 5)Fracture of the acromion process

E N D
CLASSIFICATIONThe injuries to be described may be classified as follows: Fracture of the shoulder girdle [1,2] Fractures of the clavicle 3)Fractures of the body of the scapula 4)Fractures of the neck of the scapula 5)Fracture of the acromion process 6)Fracture of the coracoid process
Injuries of the shoulder and related joints • Dislocation of the stemo-clavicular joint • Strain of the stemo-clavicular joint • Subluxation and dislocation of the acromio-clavicular joint • Strain of the acromio-clavicular joint • Dislocation of the shoulder • Rupture of the tendinous rotator cuff of the shoulder
Fractures of the humerus [1 ] fracture of the neck of the humerus [2]Fracture of the greater tuberosity Complex fractures of the upper end of the humerus [3] Fracture of the shaft [4] Supracondylar fractur [5] Fractures of the condyle [6]Fractures of the epicondyles
DISLOCATION OF THE SHOULDER The shoulder (glenohumeral) joint is dislocated commonly in adults but seldom in children. Pathology For practical purposes dislocations of the shoulder may be grouped into two main types anterior and posterior. Anterior dislocation is very much the more common. The cause is nearly always a fall onto the outstretched hand .
Fig. 11.4 Typical radiographic appearance in anterior dislocation of the shoulder
In the less common posterior dislocation there may be a history of a direct blow to the front of the shoulder, driving the humeral head backwards. More often, however, posterior dislocation is the consequence of an electric shock or an epileptiform convulsion, which perhaps acts by causing violent medial rotation. In such cases, both shoulders may be dislocated simultaneously.
Clinical features • Anterior dislocation. Pain is severe, and the patient is unwilling to attempt movements of the shoulder. • On examination, the contour of the shoulder below the tip of the acromion normally made strongly convex by the prominence of the humeral head is flattened, so that the tip of the acromion is now the most lateral point of the shoulder region. radiographic examination is always necessary. • Radiographs show that the outline of the humeral articular surface is not congruous with the articular surface of the glenoid fossa (Fig. 11.4).
An important sign of Posterior dislocationis fixed medial rotation of the arm, which cannot be rotated outwards even as far as the neutral position. There is also flattening anteriorly below the front of the acromion, where the head of the humerus normally forms a rounded bulge
Fig. 11.5 0 Anteroposterior radiograph in a case of posterior dislocation of the shoulder. Displacement is not obvious in this projection and might be overlooked, but note from the shape of its upper end that the humerus is rotated medially. This characteristic 'light bulb' appearance of the medially rotated bone is an important clue to the diagnosis. [BjThe same shoulder after reduction of the dislocation, showing normal congruity of the joint surfaces.
Treatment The dislocation should be reduced as soon as possible. An anesthetic is usually necessary. Anterior dislocation. The well-known Kocher manoeuvre may still be used; the steps (slightly modified) are as follows: (1) With the elbow flexed to a right angle, steady but gentle traction is applied in the line of the humerus. (2) The arm is rotated laterally. (3) The arm is adducted by carrying the elbow across the body towards the midline. (4) The arm is rotated medially so that the hand falls across the opposite side of the chest.
The alternative technique of reduction now widely preferred is to pull firmly and steadily upon the semi abducted arm against counter traction in the axilla, which may be provided either by an assistant or by the surgeon's stockinged foot; at the same time, direct backward pressure may be applied over the displaced humeral head by an assistant. Posterior dislocation. Reduction is effected by rotating the arm laterally while applying longitudinal traction on the arm. Direct forward pressure may also be applied over the displaced humeral head. The after treatment is the same as for anterior dislocation.
Complications 1-Injury to the axillary nerve. The axillary (circumflex) nerve is often damaged in anterior dislocations of the shoulder. 2-Paralysis of the deltoid muscle, with a small area of anaesthesia at the lateral aspect of the upper arm. 3-Vascular injury. In anterior dislocation the displaced humeral head may occasionally damage the axillary artery. 4-Associated fracture. Dislocation of the shoulder is often accompanied by fracture of the greater tuberosity of the humerus 5-Recurrent anterior dislocation of the shoulder
Diagnosis • This is largely based on the history. • Radiographic demonstration of a humeral head defect is confirmatory evidence. In a doubtful case the precise nature of the pathology may be demonstrated by computed tomographic (CT) scanning after the injection of contrast medium into the joint (Fig. 11.9), or by arthroscopy. Treatment If the disability is troublesome, operation is advised. Many operations have been advocated, but the two most commonly used both depend upon a repair of the deficient anterior tissues. In the Putti-Platt operation the subscapularis muscle is shortened to limit lateral rotation. In an alternative operation, that of Bankart, the detached capsule and glenoid labrum are reattached to the front of the glenoid rim. Arthroscopic techniques have been developed, allowing closed repair of the labrum and capsule with suture
Fig. 11.7 Horizontal section of left shoulder showing the pathology of recurrent dislocation,[a] Normal condition, [b] The humeral head is shown dislocated forwards. It has stripped the capsule from the anterior margin of the glenoid, creating a pocket in front of the neck of the scapula into which the humeral head is displaced. Note that the humeral head has been dented (arrow) by the sharp glenoid margin. The defect thus caused in the articular surface is a typical feature.
Fig. 11.8 [a] Typical defect of the articular surface of the humeral head (arrow), found in most cases of recurrent dislocation of the shoulder, [b] Radiographic appearance. The defect is seen at the upper and outer quadrant of the humeral head as a vertical edge of compacted bone (arrow). It is shown best when the arm is in medial rotation, as in this radiograph.
Fig. 11.9 CT scan of shoulder after the injection of contrast, showing a large anterior pocket where the capsule and periosteum have been stripped from the bone. Note also the small fragment detached from the anterior margin of the glenoid fossa.
FRACTURES OF THE HUMERUSFRACTURE OF THE NECK OF THE HUMERUS Fracture of the neck of the humerus occurs most often in elderly women, in whom it is a common injury. Diagnosis The fracture may easily be overlooked if it is impacted, because the patient may be able to use the arm to some extent without severe pain. The possibility of a fracture should always be suspected from the nature of the injury. Also there is extensive bruising in the upper and middle parts of the arm.
Fig. 11.12 [a] Fracture of the neck of the humerus with moderate displacement. Radiographs do not indicate with certainty whether such a fracture is impacted or not, but this is easily decided by clinical examination (see text),[|] Extensive bruising gravitating down the arm, a feature typical of these fractures.
Treatment • Standard conservative method. In the usually elderly victim of this injury, displacement should be ignored and attention concentrated on the restoration of function. Whether or not immobilization is necessary will depend upon the state of the fracture. • Impacted fractures. If the fracture is impacted, immobilization is unnecessary. Active and assisted shoulder movements should be begun immediately and continued daily, the arm being carried in a sling in the intervals between treatment.
Unimpacted fractures. If the fracture is not impacted, immediate shoulder exercises are impracticable because of the pain that movement causes. The arm should be supported in a sling, supplemented by a body bandage to hold the arm to the chest wall for the first week. • Elbow, wrist and finger exercises should be practiced from the beginning, but shoulder movements are deferred for 2 or 3 weeks, when the sling may be worn outside the clothes. By that time the fragments are generally glued together sufficiently by granulation tissue to allow assisted shoulder exercises with little or no pain, and without fear of retarding union.
Alternative surgical methods for special cases. Reduction can often be achieved by manipulation under anesthesia. To maintain reduction it is sometimes necessary to immobilize the limb on an abduction frame for 4 weeks. Operative reduction by internal fixation. The choice lies between a metal plate fixed with screws (Fig. I1.13B), or tension band wiring. replacement arthroplasty used for the damaged natural head (Fig. 11.14).
Complications • Joint stiffness. • Arterial injury. • Nerve injury. • Dislocation of the shoulder. Rarely the fracture is associated with dislocation of the shoulder
Fig. 11.14 Neerhemiarthroplasty replacing a severely comminuted fracture of the humeral head with a metal-stemmed prosthesis.