Download
1 / 34
370 likes | 805 Views
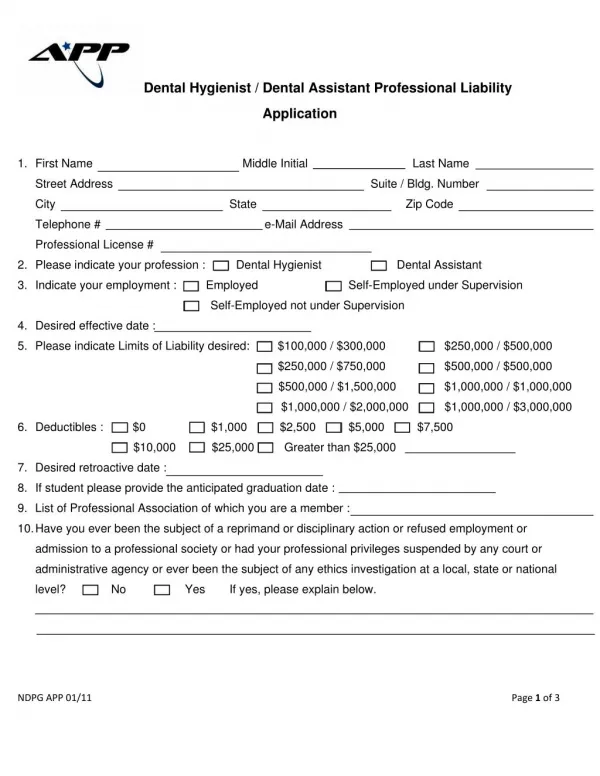
Examination of patients with partial adentia . Complications if patients have partial adentia . . Dental history. Reasons for the loss of teeth (severe dental caries – nutritional problems, advanced periodontal disease, traumatic injury or surgical excision). Health and medical history.

E N D
Examination of patients with partial adentia. Complications if patients have partial adentia.
Dental history • Reasons for the loss of teeth (severe dental caries – nutritional problems, advanced periodontal disease, traumatic injury or surgical excision)
Health and medical history • Chronic degenerative or dysfunctional diseases (diabetes, arthritis, obesity, hypertension, and osteoporosis) compromise treatment results. • Medication history - Adverse affect the oral tissues • Dietary patterns - Health problems are complicated by nutritional inadequacies; nutritional inadequacies can be compounded by poor oral health.
Subjective evaluation • Physical condition • Muscular control • Manual dexterity • Facial expressions • Tooth display • Spech patterns • Mental capacities • Dental knowledge
Patient’s record • Diagnosis • Treatment plans • Treatment provided • Progress and prognosis • Consultation request • Reaction of the patient • Laboratory work authorizations and medication prescriptions and administration
Clinical examination 1 • Oral hygiene status – control of dental plague and maintance of periodontal health are critical to the success of RPD treatment • Interproximal food impaction: vertical, which is the forceful wedging of food against the gingival tissues and into the interproximal spaces through occlusal pressure, and horizontal, which is the forcing of food between the teeth by the tongue, lips, and cheeks • Carious lesions and missing teeth – all detectable caries lesions, existing restorations – the age of certain restorations and/or prosthesis, areas of erosion or unusual abrasion; extent of dental caries activity, if it ahs been a significant problem – potential ability of the patient to control this disease
Clinical examination 2 • Periodontal health – general color and texture of the gingival tissues (healthy gingiva is pink in color, translucent, and have a dull stippled appearance with varying degree of melanin pigmentation. The color changes at the line of demarcation between attached gingival tissues and unattached mucosa. • The depth of the periodontal pockets of all remaining teeth must be measures and recorded • Periodontal Screening Record (PSR) – indicates only sextant measurements
Clinical examination 3 Degree of teeth mobility: • ■ Class 1: A tooth demonstrates greater than • normal movement, but less than 1 mm of • movement in any direction. • ■ Class 2: A tooth moves 1 mm from normal • position in any direction. • ■ Class 3: A tooth moves more than 2 mm in any • direction, including rotation or depression. A • change from normal physiologic movement • may indicate traumatic occlusion or periodontal • disease. Teeth exhibiting Class 3 mobility • have a poor prognosis and usually will require • extraction.
Clinical examination 4 • Intraoral mucosa (palate, edentulous ridges, tongue, cheeks, floor of the mouth, and vestibules) - ulcerations, inflammations, suspicious lesions. Biopsy may be required if there are any white or red lesions.If there is prosthesis – fungal infection is seen frequently, especially in the maxilla. Candida infection is frequently associated with the presence of papillary hyperplasia of the palate. • Residual alveolar ridge – visually and by palpation. The size, shape, height and location of the adjacent muscles and soft-tissue attachments are noted. The relative firmness of the overlying mucosa is palpated. Determination of flabby, movable, unsupported soft tissues over the denture-bearing area and presence of sharp bony spines or ledges of bone. Atrophic soft tissues are frequently found in elderly or malnourished patients. This mucosa is thin, smooth, and transparent, blanch readily under moderate finger pressure. This type of mucosa influences the impression technique for a final impression – unsupported tissues should not be under heavy compression using a high-viscosity impression material.
Clinical examination 5 • Tori – location and necessity in surgical modification. If the tori are large or mushroom-shaped – should be surgically removed • Occlusion - The location of any abnormal deflective occlusal contacts or prematurities should be determined and recorded on the clinical chart. • Occlusal plane - Evaluate the orientation of the occlusal plane and note teeth that have supraerupted into opposing edentulous spaces Correction of the occlusal plane discrepancy 1. Selective grinding of the cusps and/or enameloplastyof other occlusal surfaces. 2. Restoration with a crown at the proper occlusal height. 3. Gross occlusal reduction requiring subsequent restoration, often involving endodontic treatment. 4. Extraction of the tooth. • Severe vertical overlap of the anterior teeth often results in problems in the design and fitting of RPDs. Excessive anterior vertical overlap may also be a sign of posterior occlusal collapse, associated with accompanying loss of interarch space.
Clinical examination 6 • Eccentric mandibular movements – • evaluate occlusal contacts in centric relation position and maximum intercuspation, but also when the patient moves the jaw throughout lateral excursive movements. • Often, the loss of some teeth with potential drifting of adjacent remaining teeth can result in malpositionedteeth and traumatic occlusion, with mandibular guidance being forced upon weak teeth. • Signs of traumatic occlusion are: • tooth mobility or excessive attrition of the occlusal surfaces • look for evidence of bruxism or clenching; • mobile, chipped teeth, or severely worn opposing facets are possible signs of parafunctional habits
Clinical examination 7 • Existing prosthesis – • adequacy of the design • possible harmful effects resulting from poor framework fit • poor tissue adaptation • the size, type, and condition of the prosthetic teeth denture base extension • the occlusal scheme of the prosthesis • esthetic expectations • the size, form, and color of anterior prosthetic teeth • adequate support the patient ’ s facial musculature
Clinical examination 8 • Temporomandibularjoint - symptoms of pain and muscular tenderness • developmental disorders, TMJ arthritis, rheumatoid arthritis, trigeminal neuralgia, osteochondritis, osteoarthritis, posterior and anterior derangements, and referred pain must be considered in the differential diagnosis • the masseter and the internal pterygoidmuscles on one side of the jaw are most often involved. • To palpate the anterior fibers of the temporal muscle, the forefinger is placed on the cheek opposite the insertions of the muscle on the coronoid process. The other forefinger is placed inside the cheek opposite the contralateral finger. The masseter and internal pterygoidmuscles are palpated with forefingers of each hand, one on the cheek and one opposing it in the mouth. The external pterygoid muscle cannot be palpated.
Clinical examination 9 • Tongue – the size within the dental arches • Problems may occur due to protrusion outward through the edentulous spaces of the lateral borders of the tongueor • If the tongue “ overflows ” the occlusal table of the remaining mandibular teeth • Muscle tone - In patients who have lost occlusal vertical dimension and extraoral facial support because of the detrimental consequences of long - standing edentulism or inadequate prosthodontic replacement of missing teeth, a decrease in muscle size and muscle tone is evident. Thin, soft lips, narrow vermilion borders, drooping corners of the mouth, and pronounced facial wrinkles are signs of aging that accompany the progression toward edentulism. • Problems with esthetics and function are often complicated by the loss of muscle strength and tone.
Clinical examination 10 • Oral or systemic evidence of reduced tissue tolerance – related to the systemic health of the patient • When the supporting tissues deteriorate, the RPD becomes unstable and there is an increase in the destructive forces on the remaining intraoral tissues, also adding unfavorable stress on supporting abutment teeth.
Systemic conditions that have intraoral manifestations and influence the success of prosthodontic treatment 1 • Pernicious anemia - Monitor denture stability and occlusion required to minimize pressure areas. Poor denture retention results from lack of saliva. • Vitamin or nutritional deficiencies - Dietary counseling and supplementation are needed when eating habits cannot be changed. Proper base extension and stability are needed to prevent mucosal irritation. • Hypertension - Avoiding hypertensive episodes is important. Compliance with physician’s instructions and medications should be confirmed. Reduce length of appointments and provide a reassuring attitude and environment. • Diabetes - Borders should not be overextended. Patient’s mouth is prone to sore spots. Patient must maintain good tissue hygiene and employ times for tissue rest, without wearing the prosthesis. Dentist should recall patient to monitor tissue health and verify occlusion. • Osteoporosis - Patient has tendency to narrowing of maxillary ridge and broadening of mandibular ridge, leading to appearance of horizontal discrepancies, i.e., posterior “ crossbite. ” Occlusion should be evaluated and maximum coverage of residual ridges should be provided for support.
Systemic conditions that have intraoral manifestations and influence the success of prosthodontic treatment 2 • Lichen planus - Severe cases of erosive lichen planus may prevent the comfortable wearing of RPDs. • Fungal infections - Dentist should eradicate fungal lesions with antimycotictherapy before RPD is fabricated. • Postradiation therapy - Dentist must monitor fi t and correct fit when sore spots exist in a rapid manner. Overextensions should be avoided so that they do not become secondarily infected, leading to osteoradionecrosis. Xerostomiareduces patient ’ s ability • to wear removable prostheses. Occlusal vertical dimension is reduced due to muscle trismus.
Systemic conditions that have intraoral manifestations and influence the success of prosthodontic treatment 3 • Climacteric (i.e., menopausal changes) - Longer adjustment phase to RPD is required due to mucosal and psychologicchanges. • Chronic pulmonary disease (i.e., emphysema and chronic bronchitis) - Patient has little pulmonary reserve and poor reaction to stress. Dentist should keep appointments short. Occlusal vertical dimension is difficult to record because of patient’s tendency to mouth breathe. • Salivary gland disorders - Wearing the RPD becomes intolerable because of pain, burning, and frictional abrasion of the oral membranes from tissue - fitting and polished surfaces. • Neurologic disorders Bell’s palsy - Dentist should not overstretch the angle of mouth and should add sufficient bulk to buccal surface contour of maxillary RPD to support flaccid muscles.
Systemic conditions that have intraoral manifestations and influence the success of prosthodontic treatment 4 • Parkinsonism - Dentist should teach careful oral hygiene, use of tissue conditioners, and balanced occlusion. Retention is impaired from increased salivation. Maximum peripheral extension decreases denture retention. Patient lacks muscular coordination to control the prosthesis. Determination of occlusal vertical dimension is difficult because of tremor and muscle hypertonicity. • TM disturbances - History of subluxation could prohibit extensive dental procedures such as impressioning or making maxillomandibularrelation records. Frequent occlusal adjustments may be necessary.
Radiographic evaluation diagnosis • Carious lesions • Alveolar bone resorption • Bone density • Root configuration • Periodontal ligaments and the lamina dura • Radiolucent or radiopaque lesions
Analysis of the diagnostic casts • Criteria for the acceptability of diagnostic casts include the following: • 1. Anatomic details of the dental arches should be accurately reproduced, including the teeth, gingival tissues, frenum attachments, and residual ridges. • 2. There should be no dental stone nodules, voids, or artifacts in critical anatomic areas of the casts. • 3. The bases of the diagnostic casts should be 10 – 15 mm thick at the thinnest areas. • 4. The bases of the casts should be approximately parallel to the occlusal plane of the dental arch. • 5. The sides of the diagnostic cast should be neatly trimmed perpendicular to the base and a few millimeters outside the depth of the vestibular tissues. • 6. The “ tongue space ” of the mandibular cast should be clear of unnecessary dental stone, approximately level with the depth of the lingual vestibules. This can be created with ease at the time of pouring the impression by using additional alginate impression material • to “ fill ” the tongue space and render the area smooth and even with the depth of the lingual vestibules.
Evaluation of the mounted diagnostic casts • Occlusal relationships • Occlusal plane • Abutment tooth contours • Rest seat areas • Interarch space (interarch distance) • Residual ridge relation • Tissue contours
Evaluation of the patient’s psychological status four types of patients: • Philosophic • Emotional • exacting • indifferent. Evaluation of the patient’seconomic priorities
Prosthodontic Diagnostic Index (PDI) • ■ Criteria 1: Location and extent of the edentulous area(s) include four levels described as ideal or minimally compromised edentulous area (single arch), moderately compromised edentulous area (both arches), substantially compromised edentulous area, and severely compromised edentulous area. • ■ Criteria 2: Abutment conditions are described as ideal or minimally compromised abutment, moderately compromised abutment, substantially compromised abutment, and severely compromised abutment condition. • ■ Criteria 3: Occlusion includes ideal or minimally compromised occlusal characteristics, moderately compromised occlusal characteristics (some adjunctive adjustments and Angle ’ s Class I jaw/molar relation), substantially compromised occlusal characteristics (reestablishment of occlusion and Angle’s Class II jaw/molar relation), and severely compromised occlusal characteristics (reestablishment of occlusion and occlusal vertical dimension [OVD], and Angle’s Class II Div 2 and Class III jaw/molar relation). • ■ Criteria 4: Residual ridge classification follows that is used to categorize any of the edentulous areas that will be restored in the partially edentulous patient.
ACP classification system of complete edentulism • Class I • This class characterizes the stage of edentulism that is most apt to be successfully treated with complete dentures using conventional prosthodontic techniques. All 4 of the diagnostic criteria are favorable. • ■ Residual bone height of ≥ 21 mm measured at the least vertical height of the mandible on a panoramic radiograph • ■ Residual ridge morphology resistant to horizontal and vertical movement of the denture base; type A maxilla • ■ Location of muscle attachments conducive to denture base stability and retention; type A or B mandible • ■ Class I maxillomandibular relationship
Class II • This class is distinguished by the continued physical degradation of the denture-supporting anatomy. It is also characterized by the early onset of systemic disease interactions and by specific patient management and lifestyle considerations. • ■ Residual bone height of 16 to 20 mm measured at the least vertical height of the mandible on a panoramic radiograph • ■ Residual ridge morphology resistant to horizontal and vertical movement of the denture base; type A or B maxilla • ■ Location of muscle attachments with limited influence on denture base stability and retention; type A or B mandible • ■ Class I maxillomandibular relationship • ■ Minor modifiers, psychosocial considerations, mild systemic disease with oral manifestations
Class III • This class is characterized by the need for surgical revision of supporting structures to allow for adequate prosthodontic function. Additional factors now play a significant role in treatment outcomes. • ■ Residual alveolar bone height of 11 to 15 mm measured at the lease vertical height of the mandible on a panoramic radiograph • ■ Residual ridge morphology with minimum influence to resist horizontal or vertical movement of the denture base; type C maxilla • ■ Location of muscle attachments with moderate influence on denture base stability and retention; type C mandible • ■ Class I, II, or III maxillomandibular relationship • ■ Conditions requiring preprosthetic surgery • ■ Minor soft tissue procedures • ■ Minor hard tissue procedures including aveoloplasty • ■ Simple implant placement; no augmentation required • ■ Multiple extractions leading to complete edentulism for immediate denture placement • ■ Limited interarch space (18 to 20 mm) • ■ Moderate psychosocial considerations and/or moderate oral manifestations of systemic diseases or conditions such as xerostomia • ■ TMD symptoms • ■ Large tongue (occludes interdental space) with or without hyperactivity • ■ Hyperactive gag reflex
Class IV • This class represents the most debilitated edentulous condition. Surgical reconstruction is almost always indicated but cannot always be accomplished because of the patient’s health, preferences, past dental history, and financial considerations. When surgical revision is not an option, prosthodontic techniques of a specialized nature must be used to achieve an adequate outcome. • ■ Residual vertical bone height of ≤ 10 mm measured at the least vertical height of the mandible on a panoramic radiograph • ■ Class, I, II, or III maxillomandibular relationships • ■ Residual ridge offering no resistance to horizontal or vertical movement; type D maxilla • ■ Muscle attachment location that can be expected to have significant influence on denture base stability and retention; type D or E mandible • ■ Major conditions requiring preprosthetic surgery • ■ Complex implant placement, augmentation required • ■ Surgical correction of dentofacial deformities required • ■ Hard tissue augmentation required • ■ Major soft tissue revision required, that is, vestibular extensions with or without soft tissue grafting
■ History of paresthesia or dysesthesia • ■ Insufficient interarch space necessitating surgical correction • ■ Acquired or congenital maxillofacial defects • ■ Severe oral manifestation of systemic disease or conditions such as sequelae from oncologic treatment • ■ Maxillomandibular ataxia (incoordination) • ■ Hyperactivity of tongue possibly associated with a retracted tongue position and/or its associated morphology • ■ Hyperactive gag reflex managed with medication • ■ Refractory patient (a patient who presents with chronic complaints following appropriate therapy), who may continue • to have difficulty achieving their treatment expectations despite the thoroughness or frequency of the treatments • provided • ■ Psychosocial conditions warranting professional intervention
Type A maxilla • Hard palate form • Anterior maxilla • Maxillary tuberosities • Anterior labial and posterior buccal vestibular depth that resists vertical and horizontal movement of the denture base • Palatal morphology that resists vertical and horizontal movement of the denture base • Sufficient tuberosity definition that resists vertical and horizontal movement of the denture base • Hamular notch is well defined to establish the posterior extension of the denture base
Type B maxilla • Hard Palate form • Residual Alveolar Ridge • – Anterior • – Posterior • Maxillary Tuberosities • Loss of posterior buccal vestibule • • Tuberosity and hamular notch are poorly defined compromising delineation of the posterior extension of the denture base • • Maxillary palatal and/or lateral tori are rounded and do not affect the posterior extension of the denture base • • Palatal vault morphology that resists vertical and horizontal movement of the denture base
Type C maxilla • Hard Palate form • Anterior Maxilla • Maxillary Tuberosities • Loss of anterior labial vestibule • Prominent midline suture • Maxillary palatal and/or lateral tori with bony undercuts that do not affect the posterior extension of the denture base • Hyperplastic, mobile anterior ridge that offers minimum support and stability of the denture base • Palatal vault morphology that offers minimal resistance to vertical and horizontal movement of the denture base • Reduction of the post malar space by the coronoid process during mandibular opening and/or excursive movements
Type D maxilla • Hard Palate form • •Residual alveolar ridge • – Anterior • – Posterior • Maxillary Tuberosities • Loss of anterior labial and posterior buccal vestibules • Maxillary palatal and/or lateral tori-rounded or undercut- that interferes with the posterior border of the denture • Hyperplastic, redundant anterior ridge • Palatal vault morphology that does not resist vertical or horizontal movement of the denture base • Prominent anterior nasal spine
Type E maxilla • No attached mucosa in any region • Cheek and lip movement = tongue movement