Download
1 / 12
130 likes | 360 Views
Dharamshila Hospital and Research Centre (DHRC) is totally committed and focused in its fight against cancer since 1994. We take pride in touching and enriching lives with love, compassion, a positive attitude and following ethical practices based on transparency and accountability.

E N D
Head And Neck Cancer For More Information : www.dharamshila.com
Head And Neck Cancer Information on cancers of the head and neck, including their symptoms, how they are diagnosed, treatments you might have, possible side effects and how to get further support. Head and Neck cancers are the commonest cancer in Men. Unfortunately, even young adults are being diagnosed with the disease because more and more children are using pan masala / Gutka and other tobacco products. Inspite of the fact that head and neck cancers are completely preventable, the incidence is rising at an alarming speed. By Early detection and optimum treatment, it is possible to cure all the above cancers.
TYPES OF HEAD AND NECK CANCERS ? • About 90% head and neck cancers begin in the cells that line the mucosal surfaces in the head and neck area, e.g., mouth, nose, and throat. Mucosal surfaces are moist tissues lining hollow organs and cavities of the body open to the environment. Normal mucosal cells look like scales (squamous) under the microscope, so head and neck cancers are often referred to as squamous cell carcinomas. • Head and neck cancers can also develop from other types of cells: • Lymphomas develop from the cells of the lymphatic system. • Adenocarcinomas develop from cells that form the lining of glands in the body. • Sarcomas develop from the cells which make up muscles, cartilage or blood vessels. • Melanomas start from cells called melanocytes, which give colour to the eyes and skin. • Cancers of the head and neck are further identified by the area in which they begin: • Oral Cavity / Mouth Cancer • Paranasal sinuses and nasal cavity> • Pharynx - Nasopharynx - Oropharynx - Hypopharynx • Salivary glands • Lymph nodes in the upper part of the neck • You can see information on cancer of the Larynx
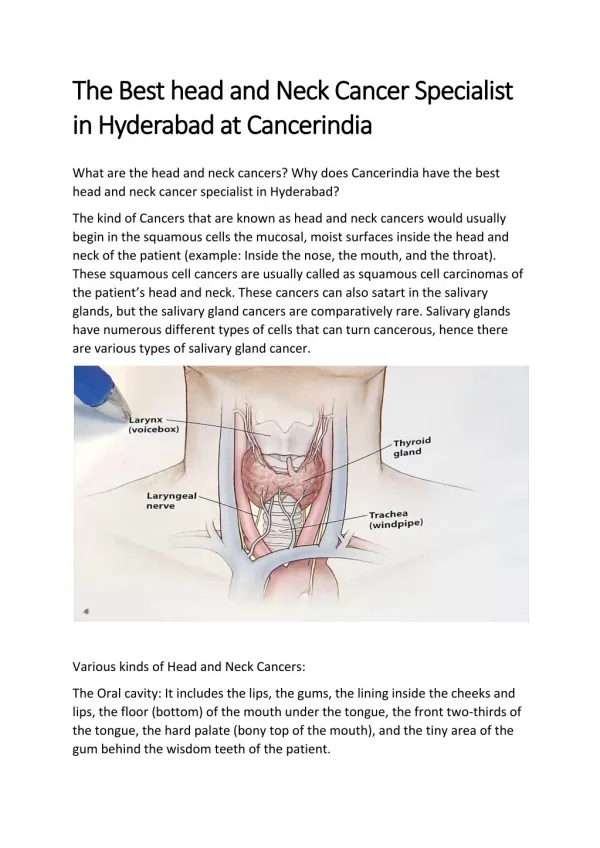
Oral cavity. The oral cavity includes the lips, the front two-thirds of the tongue, the gingival (gums), the buckle mucosa (lining inside the cheeks and lips), the floor (bottom) of the mouth under the tongue, the hard palate (bony top of the mouth), and the small area behind the wisdom teeth. • Para nasal sinuses and nasal cavity. The par nasal sinuses are small hollow spaces in the bones of the head surrounding the nose. The nasal cavity is the hollow space inside the nose. • Pharynx. The pharynx is a hollow tube about 5 inches long that starts behind the nose and leads to the esophagus (the tube that goes to the stomach) and the trachea (the tube that goes to the lungs). The pharynx has three parts: • - Nasopharynx. The Nasopharynx, the upper part of the pharynx, is behind the nose. • - Or pharynx. The or pharynx is the middle part of the pharynx. The Oropharynx includes the soft palate (the back of the mouth), the base of the tongue, and the tonsils. • - Hypo pharynx. The hypo pharynx is the lower part of the pharynx. • Salivary glands. The salivary glands produce saliva, the fluid that keeps mucosal surfaces in the mouth and throat moist. There are many salivary glands; the major ones are in the floor of the mouth, and near the jawbone. • Lymph nodes in the upper part of the neck. Sometimes, squamous cancer cells are found in the lymph nodes of the upper neck when there is no evidence of cancer in other parts of the head and neck. When this happens, the cancer is called metastatic squamous neck cancer with unknown (occult) primary. • Larynx. The larynx, also called the voice box, is a short passageway formed by cartilage just below the pharynx in the neck. The larynx contains the vocal cords. It also has a small piece of tissue, called the epiglottis, which moves to cover the larynx to prevent food from entering the air passages. • Cancers of the brain, eye, and thyroid as well as those of the scalp, skin, muscles, and bones of the head and neck are not usually grouped with cancers of the head and neck.
HEAD AND NECK CANCERS Symptoms • Oral cavity • - Raised growth, swelling or lump • - Changes in colour – red, brown, white or black spots / patches • - Continuous bleeding or a sore which does not heal • - Tingling, burning or numbness in tongue or lip • - Pain anywhere in the mouth • - Painful, sensitive or loose teeth • - Difficulty in swallowing or talking • Nasal cavity and sinuses • - Blocked sinus, chronic sinus infections, not responding to antibiotics • - Nose bleeds • Pharynx • - Ear pain, Difficulty in hearing • - Difficulty in breathing & Speaking • - Frequent headaches • - Pain or ringing in the ears • Larynx • - Hoarseness of Voice • - Difficulty in Swallowing • - Ear pain • Oesophagus • - Difficulty in swallowing solid food • Salivary Gland and Thyroid • - Lump or Swelling in the neck
HEAD AND NECK CANCER DIAGNOSIS AND STAGING WORK UP • To find the cause of symptoms, a surgical oncologist evaluates a person's medical history, performs a physical examination, and orders diagnostic tests. The exams and tests conducted may vary depending on the symptoms. Examination of a sample of tissue under the microscope is always necessary to confirm a diagnosis of cancer. • Some exams and tests that may be useful are as under : • Physical examination may include visual inspection of the oral and nasal cavities, neck, throat, and tongue using a small mirror and/or lights. The surgical oncologist may also feel for lumps in the neck, lips, gums, and cheeks. • Endoscopy is the use of a thin, lighted tube called an endoscope to examine areas inside the body. The type of endoscope the Surgical Oncologist uses depends on the area being examined. For example, a laryngoscope is inserted through the mouth to view the larynx; an esophagoscope is inserted through the mouth to examine the esophagus; and a nasopharyngoscope is inserted through the nose so that the surgical oncologist can see the nasal cavity and nasopharynx. • Laboratory tests examine samples of blood, urine, or other substances from the body. • X-rays create images of areas inside the head and neck on film. • CT scan is a series of detailed pictures of areas inside the head and neck created by a computer linked to an x-ray machine. • Magnetic resonance imaging (or MRI) uses a powerful magnet linked to a computer to create detailed pictures of areas inside the head and neck. • PET scan uses sugar that is modified in a specific way so it is absorbed by cancer calls and appears as dark areas on the scan.
The stage of a cancer is a term used to describe its size and whether it has spread beyond its original site. Knowing the extent of the cancer helps the doctors to decide on the most appropriate treatment. • A common way of staging head and neck cancers is the TNM staging system. • T describes the size of the tumor and whether it has begun to spread to nearby structures, such as the skin or muscle. • N describes whether the cancer has spread to the lymph nodes. • M describes whether the cancer has spread to another part of the body (secondary or metastatic cancer). • The staging of the different types of head and neck cancers are all slightly different. Your doctor or nurse can give you more details about the stage of your cancer. • Grading Grading refers to the appearance of the cancer cells under the microscope. The grade gives an idea of how quickly the cancer may develop. Squamous cell cancers of the head and neck are graded from 1–3. • Low-grade or grade 1 means that the cancer cells look very like normal cells in the head and neck area. • In high-grade or grade 3 cancers the cells look very abnormal and are more likely to spread. • Moderate-grade or grade 2 cancers fall between these two grades and have a level of activity somewhere between. • Biopsy is the removal of tissue. A pathologist studies the tissue under a microscope to make a diagnosis. A biopsy is the only sure way to tell whether a person has cancer. If the diagnosis of cancer is confirmed, the surgical oncologist will want to know the stage (or extent) of disease. Staging is a careful attempt to find out whether the cancer has spread and, if so, to which parts of the body. Staging may involve an examination under anesthesia (in the operating room), x-rays and other imaging procedures, and laboratory tests. Knowing the stage of the disease helps the surgical oncologist plan treatment. Staging of head and neck cancer
HEAD AND NECK CANCER TREATMENT • Tumour Board Evaluation Each and every Head and Neck cancer patient is evaluated by a special team of surgical oncologists (Head & Neck unit), medical oncologists, Radiation Oncologists, Onco-pathologists and Imaging Specialists. Depending on the age, general condition, type of pathology and stage of the disease, a custom made treatment plan is charted out for each and every patient as per International Treatment Guidelines. • Modalities of Treatment Available for Head and Neck Cancers • - Surgery • - Radiation • - Chemotherapy • - Rehabilitation • The treatment plan for an individual patient depends on a number of factors, including the exact location of the tumor, the stage of the cancer, and the person's age and general health. The patient and the surgical oncologist should consider treatment options carefully. They should discuss each type of treatment and how it might change the way the patient looks, talks, eats, or breathes. • SURGERY • The surgeon may remove the cancer and some of the healthy tissue around it. Lymph nodes in the neck may also be removed (lymph node dissection), if the Surgical Oncologist suspects that the cancer has spread. Surgery may be followed by radiation treatment. • Head and neck surgery often changes the patient's ability to chew, swallow, or talk. The patient may look different after surgery, and the face and neck may be swollen. The swelling usually goes away within a few weeks. However, lymph node dissection can slow the flow of lymph, which may collect in the tissues; this swelling may last for a long time. After a laryngectomy (surgery to remove the larynx), parts of the neck and throat may feel numb because nerves have been cut. If lymph nodes in the neck were removed, the shoulder and neck may be weak and stiff. Patients should report any side effects to their Surgical Oncologist or nurse, and discuss what approach to take. • Department of Surgical Oncology at Dharamshila Hospital Research Centre is pioneer in performing challenging Head and Neck Cancer Surgeries. These are not being performed by any other cancer centre in North India with such high success rate. The main objective of these surgeries is to restore normal facial appearance, chewing, swallowing and speech, ensuring a cancer free good quality of life. To know, why Head and Neck Cancer Surgeries are challenging. Read More……..
RADIATION THERAPY • Radiation therapy is also called radiotherapy. This treatment involves the use of high-energy beams to kill cancer cells. Radiation may be given with linear accelerator (external radiation therapy). It can also be given from radioactive materials placed directly into or near the area where the cancer cells are found (internal radiation therapy or Brach therapy). • In addition to its desired effect on cancer cells, radiation therapy often causes unwanted effects. Patients who receive radiation to the head and neck may experience redness, irritation, and sores in the mouth; a dry mouth or thickened saliva; difficulty in swallowing; changes in taste; or nausea. Other problems that may occur during treatment are loss of taste, which may decrease appetite and affect nutrition, and earaches (caused by hardening of the ear wax). Patients may also notice some swelling or drooping of the skin under the chin and changes in the texture of the skin. The jaw may feel stiff and patients may not be able to open their mouth as wide as before treatment. Patients should report any side effects to their Oncologist or nurse and ask how to manage these effects. • Dharamshila Hospital has commissioned a world class Elekta Synergy with VMAT Technology linear accelerator which can give radiation at 1/10th the dose being given by conventional linear accelerator. This technology minimizes the above mentioned side effects. • CHEMOTHERAPY • Chemotherapy, also called anticancer drugs. This treatment is used to kill cancer cells throughout the body. The side effects of chemotherapy depend on the drugs that are given. In general, anticancer drugs affect rapidly growing cells, including blood cells that fight infection, cells that line the mouth and the digestive tract, and cells in hair follicles. As a result, patients may have side effects such as lower resistance to infection, sores in the mouth and on the lips, loss of appetite, nausea, vomiting, diarrhoea, and hair loss. They may also feel unusually tired and experience skin rash and itching, joint pain, loss of balance, and swelling of the feet or lower legs. Patients should talk with their medical oncologist or nurse about the side effects they are experiencing, and how to handle them. There are very few side effects with modern chemotherapy protocols at Dharamshila Hospital.
HEAD AND NECK CANCER PREVENTION • EARLY DETECTION • The earlier cancer is detected the better are the chances of cure and complete recovery. It is important to realize that many cancers today are curable. • Monthly self examination by each and every one of us will go a long way in detecting cancer at the early stage. One can stand in front of large mirror and look for the following : - • Mouth : Change in colour of gums, lips and cheeks, White, Brown or red patches, ulcer, sore or scab, thickening in any part of the oral cavity. • Neck : Look for any lump, swelling or any other abnormality. • If you find anything abnormal, record it on a notebook and report it to your doctor. In case everything is normal, RELAX! • ANNUAL HEALTH CHECK UP • For Head and Neck Cancer Dental and ENT Check up is must for both the sexes. In case of suspicion, one should go for Endoscopy, biopsy, X-Ray, CT – Scan, MRI, PET CT • This is most important for all of us because it is through these annual check ups that we can find out about the status of our health. • HOW TO PREVENT HEAD AND NECK CANCERS? • Avoid active and passive smoking. • Avoid Tobacco and Tobacco Products like Gutkha, Paan, Khaini, Surti, Beedi, Cigarette
Avoid Alcohol • Maintain Good oral and dental hygiene • All smokers and tobacco chewers need several counselling sessions to leave the habit and ensure they do not start taking tobacco, after quitting it. CAUSES / RISK FACTORS • Eighty-five percent of head and neck cancers are linked to tobacco use. People who use both tobacco and alcohol are at greater risk for developing these cancers than people who use either tobacco or alcohol alone. • Other risk factors for cancers of the head and neck include the following: • Oral cavity Sun exposure (lip); poor oral hygiene, possibly human papillomavirus (HPV) infection. There are certain stages before development of frank cancer which present as White patches (leukoplakia) in the mouth which do not get rubbed off or Red patches (Erythroplakia). • Salivary glands. Radiation to the head and neck. This exposure can come from diagnostic x-rays or from radiation therapy for noncancerous conditions or cancer. • Paranasal sinuses and nasal cavity. Certain industrial exposures, such as wood or nickel dust inhalation. Tobacco and alcohol use may play less of a role in this type of cancer. • Nasopharynx. Exposure to wood dust; and consumption of certain preservatives or salted foods. • Oropharynx. Poor oral hygiene; HPV infection and the use of mouthwash that has high alcohol content are possible, but not proven, risk factors. • Hypopharynx. Plummer-Vinson (also called Paterson-Kelly) syndrome, a rare disorder that results from iron and other nutritional deficiencies. This syndrome is characterized by severe anemia and leads to difficulty swallowing due to webs of tissue that grow across the upper part of the esophagus. • Larynx. Exposure to airborne particles of asbestos, especially in the workplace. • More than 5 million children in India are addicted to gutkha, a smokeless tobacco product that is a key driver behind the country's soaring oral cancer rates. People who are at risk for head and neck cancers should come to us for check ups and learn to reduce their risk. They should also discuss how often to have checkups.
Contact Us Dharamshila Hospital And Research Centre (Your Partner in Cancer Care)Vasundhara Enclave, Near New Ashok Nagar Metro StationDelhi – 110096 (India)Patient Helpline : +91-8130000120, +91-11-43066353E-mail ID : contact@dharamshila.com