Download
1 / 57
570 likes | 573 Views
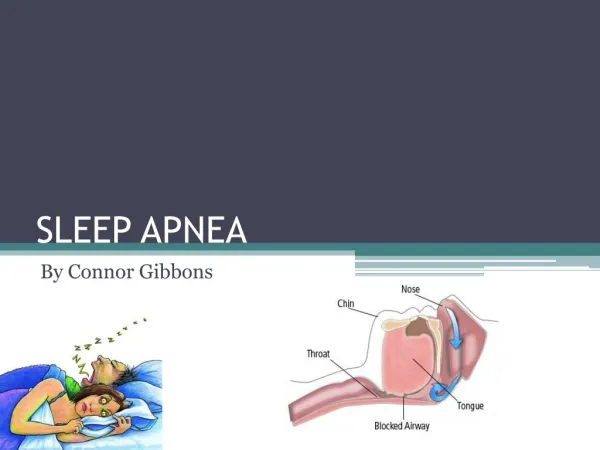
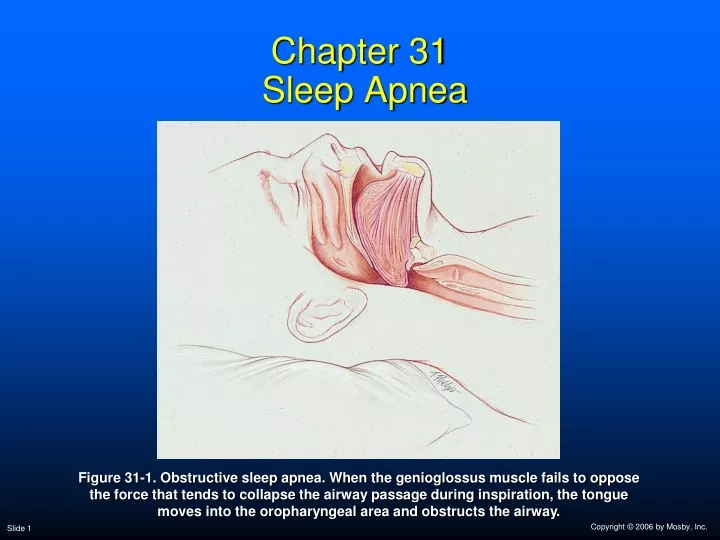
Chapter 31 Sleep Apnea. Figure 31-1. Obstructive sleep apnea. When the genioglossus muscle fails to oppose the force that tends to collapse the airway passage during inspiration, the tongue moves into the oropharyngeal area and obstructs the airway. Sleep Apnea.

E N D
Chapter 31 Sleep Apnea Figure 31-1. Obstructive sleep apnea. When the genioglossus muscle fails to oppose the force that tends to collapse the airway passage during inspiration, the tongue moves into the oropharyngeal area and obstructs the airway.
Sleep Apnea Despite the fact that the clinical manifestations of sleep apnea have be described for centuries, it was not until the early 1980s that it became acknowledged by the medical community
Stages of Sleep and Characteristic Cardiopulmonary Patterns • Two major sleep stages during normal sleep • Non–rapid eye movement (non-REM) sleep • Quiet or slow-wave sleep • Rapid eye movement (REM) sleep • Active or dreaming sleep
Non-REM Sleep • Usually begins immediately after dozing off • Four stages of non-REM sleep • Each progressing into a deeper sleep
Stages 1 and 2 • The ventilatory rate and tidal volume continually increase and decrease—brief periods of apnea may occur • The ECG shows increased slow-wave activity and loss of alpha rhythm • Cheyne-Stokes respiration is common in older adult males, especially at high altitudes
Stages 3 and 4 • Ventilation becomes slow and regular • Minute ventilation is commonly 1 to 2 L/min less than during the quiet wakeful state • Typically the: • PaCO2 levels are higher (4-8 mm Hg) • PaO2 levels are lower (3-10 mm Hg) • pH is lower (0.03-0.05 unit)
Stages 3 and 4 • Normally, non-REM sleep lasts 60 to 90 minutes • Typically, an individual moves in and out of all4 stages during non-REM sleep • Most of the time is spent in stage 2
Stages 3 and 4 • An individual may move into REM sleep, at any time, directly, from any of the 4 non-REM sleep stages • The lighter 1 and 2 stages, however, are the most common levels just before REM sleep
REM Sleep • During this period, sudden burst of fast alpha rhythms • Ventilatory rate becomes rapid and shallow • Sleep-related hypoventilation and apnea are commonly seen during this period
REM Sleep • In normal adults, apneic periods occur as often a five times per hour • These apneic periods may last 15 to 20 seconds with no discernible effects • In normal infants: • Apneas are shorter—about 10 seconds long
REM Sleep • A marked reduction occurs in the: • Hypoxic ventilatory response • Hypercapnic ventilatory response • The heart rate becomes irregular • The eyes move rapidly and dreaming occurs
REM Sleep • Paralysis of the skeletal muscles occurs • Arms • Legs • Intercostal and upper airway muscles • The diaphragm is NOT affected
Muscle Paralysis during REM Sleep Affects Ventilation in Two Ways • Paradoxical motion of the rib cage • Causes in tissue to move inward during inspiration • This causes the FRC to decrease • Loss of muscle tone in the: • Posterior muscles of the pharynx • Genioglossus—protrudes the tongue • Posterior cricoarytenoid—abducts the vocal cords
Loss of Muscle Tone in the Upper Airway May Result in Airway Obstruction • The negative pharyngeal pressure produced when the diaphragm contracts during inspiration tends to: • Bring the vocal cords together • Collapse the pharyngeal wall • Suck the tongue back into the oral pharyngeal cavity
REM Sleep • REM sleep lasts about 5 to 40 seconds • Recurs about every 60 to 90 minutes • REM sleep lengthens and becomes more frequent toward the end of a sleep period
REM Sleep • REM sleep constitutes about 20% to 25% of sleep time • It is usually more difficult to awaken a subject during REM sleep
Types of Sleep Apnea • Apnea—the cessation of breathing for 10 seconds or longer • Sleep apnea—more than five episodes of apnea per hour • May occur in either or both non-REM and REM sleep, over a 6-hour period
Types of Sleep Apnea • Generally, the episodes of apnea are more frequent and severe during REM sleep and in the supine body position • Apnea periods last more than 10 seconds and occasionally exceed 100 seconds in length • In severe cases, as many as 500 apnea periods per night may occur
Types of Sleep Apnea • Sleep apneas may appear in all age groups • In infants, it may play a role in sudden infant death syndrome (SIDS)
Obstructive Sleep Apnea(OSA) • Most common • During periods of OSA, the: • Patient, initially, appears quiet and still • Followed by an increased effort to inhale
Obstructive Sleep Apnea • OSA often ends only after an intense struggle • Snorting is often heard during periods of OSA • Called “fricative breathing” • In severe cases, the patient may: • Suddenly awaken • Sit upright in bed, and • Gasp for air
Obstructive Sleep Apnea • OSA patients usually breathe normally during wakeful periods • OSA seen more often in males than females (8:1 ratio) • Between 1% and 4% of male population • Commonly seen in obese people with short necks
Pickwickian Syndrome • Named after a character in Charles Dickens’ The Posthumous Papers of the Pickwick Club (1837) • Joe: the fat boy who snored and had excessive daytime sleepiness • Charles Dickens’ description of Joe included many of the classic features now recognized as OSA
Pickwickian Syndrome However, many patients with OSA are NOT obese, thus clinical suspicion should not be limited to this group
Some Clinical Disorders Associated with OSA • Obesity • Anatomic narrowing of the upper airway • Excessive pharyngeal tissue • Enlarged tonsils or adenoids • Deviated nasal septum • Laryngeal stenosis
Some Clinical Disorders Associated with OSA • Laryngeal web • Pharyngeal neoplasms • Micrognathia • Macroglossia • Goiter • Hypothyroidism
Some Clinical Disorders Associated with OSA • Testosterone administration • Myotonic dystrophy • Shy-Drager syndrome • Down syndrome
General Clinical Manifestations Associated with OSA • Chronic loud snoring • Hypertension • Morning headaches • Systemic hypertension • Nausea • Dry mouth on awakening • Intellectual and personality changes
General Clinical Manifestations Associated with OSA • Depression • Sexual impotence • Nocturnal enuresis • Excessive daytime sleepiness • Car accidents or job malperformance related to sleepiness • Pulmonary hypertension
Polysomnographic Monitoring Findings • Apnea-related oxygen desaturation • More than five obstructive apneas of more than 10 seconds per hour of sleep, and one or more of the following: • Frequent arousal from the apneas • PVCs • Profound bradycardia and/or asystole • Shortened sleep latency
Central Sleep Apnea • Occurs when respiratory centers of the medulla fail to send signals to the respiratory muscles • Characterized by cessation of airflow at the nose and mouth with absence of diaphragmatic excursions • Associated with cardiovascular, metabolic, or central nervous system disorders
Central Sleep Apnea Diagnosed when the frequency of apnea episodes is more than 30 in a 6-hour period
Clinical Disorders Associated with Central Sleep Apnea • Congestive heart failure • Metabolic alkalosis • Idiopathic hypoventilation syndrome • Encephalitis • Brainstem neoplasm • Brainstem infarction • Bulbar poliomyelitis • Cervical cordotomy • Spinal surgery • Hypothyroidism
General Noncardiopulmonary Clinical Manifestations • Tendency to be of normal weight • Mild snoring • Insomnia • Some of the following may also occur • Daytime fatigue • Depression • Sexual dysfunction
Mixed Sleep Apnea • Combination of obstructive and central sleep apnea • Usually begins as central sleep apnea, followed by: • Ventilatory efforts without airflow—OSA • Clinically, mixed sleep apnea is usually classified and treated as OSA
Figure 31-2. Patterns of airflow, respiratory efforts (reflected through the esophageal pressure), and arterial oxygen saturation produced by central, obstructive, and mixed apneas.
Diagnosis • Begins with a careful history • Noting presence of snoring, sleep disturbance, and daytime sleepiness • Followed by examination of upper airway and PFT to determine presence of upper airway obstruction • Blood evaluation • Polycythemia • Thyroid function • ABGs
Diagnosis • Chest radiograph • Electrocardiogram to determine: • Presence of pulmonary hypertension • State of right and left ventricular compensation • Presence of any other cardiopulmonary disease
Diagnosis and Type of Apnea • Confirmed with the following: • Polysomnographic sleep studies, which include: • EEG and EOG—to identify sleep stages • Airflow monitor • ECG • Monitor of patient’s ventilatory rate and effort • Oximetry • CT scan
Overview of the Cardiopulmonary Clinical Manifestations Associated with SLEEP APNEA
Arterial Blood Gases Severe Sleep Apnea • Chronic ventilatory failure with hypoxemia • pH PaCO2 HCO3- PaO2 • Normal (Significantly)
Time and Progression of Disease Disease Onset Alveolar Hyperventilation Chronic Ventilatory Failure 100 Point at which disease becomes severe and patient begins to become fatigued 90 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 80 70 PaCO2 Pa02 or PaC02 60 50 40 30 PaO2 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute ventilatory failure.
Acute Ventilatory Changes on Chronic Ventilatory Failure • Acute alveolar hyperventilation on chronic ventilatory failure • Acute ventilatory failure on chronic ventilatory failure
Oxygenation Indices QS/QT DO2 VO2 C(a-v)O2 Normal Normal O2ER SvO2
Hemodynamic Indices (Severe) CVP RAP PAPCWP CO SV SVICI RVSWI LVSWI PVRSVR
Radiologic Findings Chest radiograph • Right- or left-sided heart failure
Cardiac Arrhythmias • Sinus arrhythmia • Sinus bradycardia • Sinus pauses • Atrioventricular block • Premature ventricular contractions • Ventricular tachycardia